

Outcomes and Complications After All-Epiphyseal Anterior Cruciate Ligament Reconstruction in Skeletally Immature Patients
- PMID: 28451597
- PMCID: PMC5400138
- DOI: 10.1177/2325967117693604
Outcomes and Complications After All-Epiphyseal Anterior Cruciate Ligament Reconstruction in Skeletally Immature Patients
Abstract
Background: The safest and most effective technique for anterior cruciate ligament (ACL) reconstruction in skeletally immature patients is currently unknown.
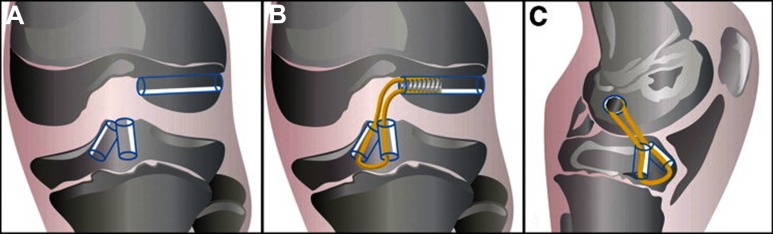
Purpose: To evaluate the functional and patient-reported outcomes of a specific all-epiphyseal ACL reconstruction technique in which the graft, bone tunnels, and fixation do not cross the knee growth plates.
Study design: Case series; Level of evidence, 4.
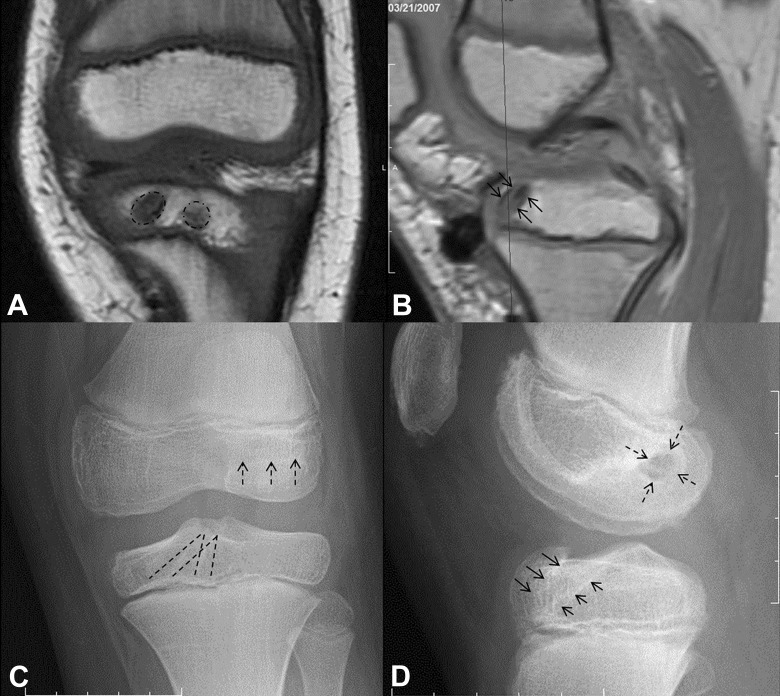
Methods: Twenty-seven patients (23 boys, 4 girls; mean age, 11 years; range, 8-15 years) underwent an all-epiphyseal ACL reconstruction with a single femoral transverse epiphyseal tunnel and primarily split tibial epiphyseal tunnels. Outcomes were evaluated in terms of the manual Lachman test, range of motion, pain, return to activity, angular or leg-length deformity on imaging, and International Knee Documentation Committee (IKDC) or Pedi-IKDC score an average of 3.8 years postoperatively, with a minimum 2-year follow-up.
Results: The mean IKDC score was 94 ± 11. There were no growth arrests, but 3 patients had knee overgrowth, and 2 required a subsequent guided growth procedure. The ACL graft failed in 4 patients (15%), and 2 patients had contralateral ACL tears (7%). There were 5 subsequent ipsilateral meniscal tears, 4 of which were retears of a repaired meniscus. Ipsilateral knee reinjury significantly correlated with the number of associated injuries at the time of index surgery (P = .040) and the number of sports played (P = .029).
Conclusion: All-epiphyseal ACL reconstruction resulted in excellent long-term functional outcomes, despite a high rate of complications (48%) and secondary procedures (37%) in this highly active cohort. The incidence of graft failure was similar to other standard ACL reconstruction techniques for patients younger than 20 years.
Keywords: ACL; all-epiphyseal; growth plate; pediatric sports medicine; physis; reconstruction.
Conflict of interest statement
One or more of the authors has declared the following potential conflict of interest or source of funding: E.J.W. is a paid consultant for and holds an ACL patent with OrthoPediatrics.
Figures

References
-
- Aichroth P, Patel D, Zorrilla P. The natural history and treatment of rupture of the anterior cruciate ligament in children and adolescents. Bone Joint J. 2002;84:38–41. - PubMed
-
- Anderson AF. Transepiphyseal replacement of the anterior cruciate ligament in skeletally immature patients. J Bone Joint Surg Am. 2003;85:1255–1263. - PubMed
-
- Angel KR, Hall DJ. Anterior cruciate ligament injury in children and adolescents. Arthroscopy. 1989;5:197–200. - PubMed
-
- Demange MK, Camanho GL. Nonanatomic anterior cruciate ligament reconstruction with double-stranded semitendinosus grafts in children with open physes: minimum 15-year follow-up. Am J Sports Med. 2014;42:2926–2932. - PubMed
-
- Dumont GD, Hogue GD, Padalecki JR, Okoro N, Wilson PL. Meniscal and chondral injuries associated with pediatric anterior cruciate ligament tears: relationship of treatment time and patient-specific factors. Am J Sports Med. 2012;40:2128–2133. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
