

Disruption of the leptomeningeal blood barrier in neuromyelitis optica spectrum disorder
- PMID: 28451627
- PMCID: PMC5400808
- DOI: 10.1212/NXI.0000000000000343
Disruption of the leptomeningeal blood barrier in neuromyelitis optica spectrum disorder
Abstract
Objective: To describe leptomeningeal blood-barrier impairment reflected by MRI gadolinium-enhanced lesions in patients with aquaporin-4 immunoglobulin G (AQP4-IgG)-positive neuromyelitis optica spectrum disorder (NMOSD).
Methods: A retrospective case series of 11 AQP4-IgG-positive NMOSD patients with leptomeningeal enhancement (LME) were collected from 5 centers. External neuroradiologists, blinded to the clinical details, evaluated MRIs.
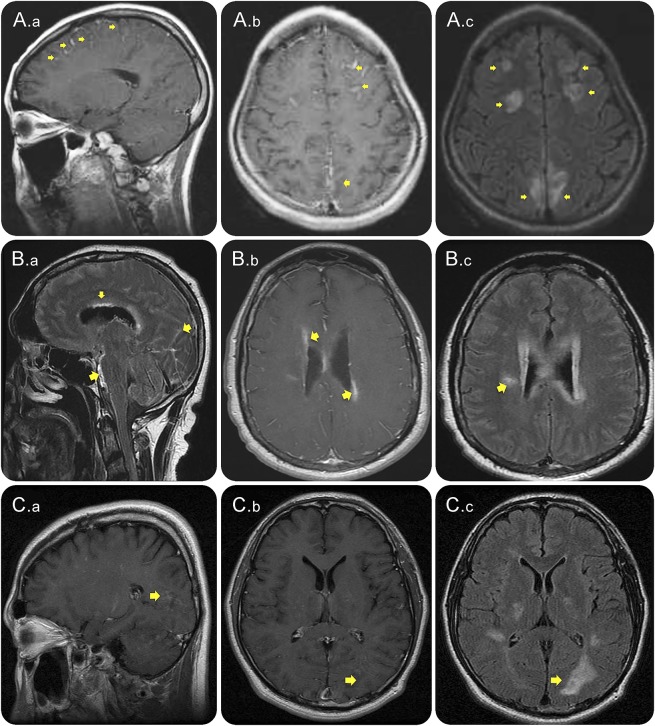
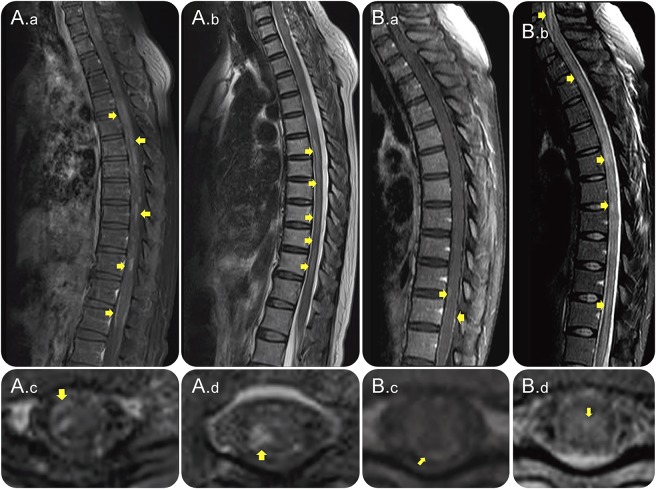
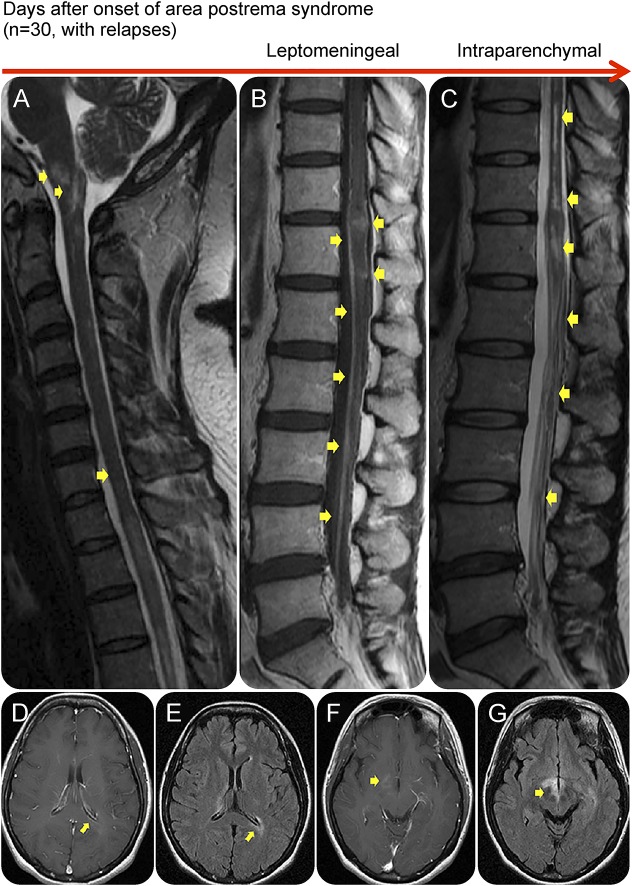
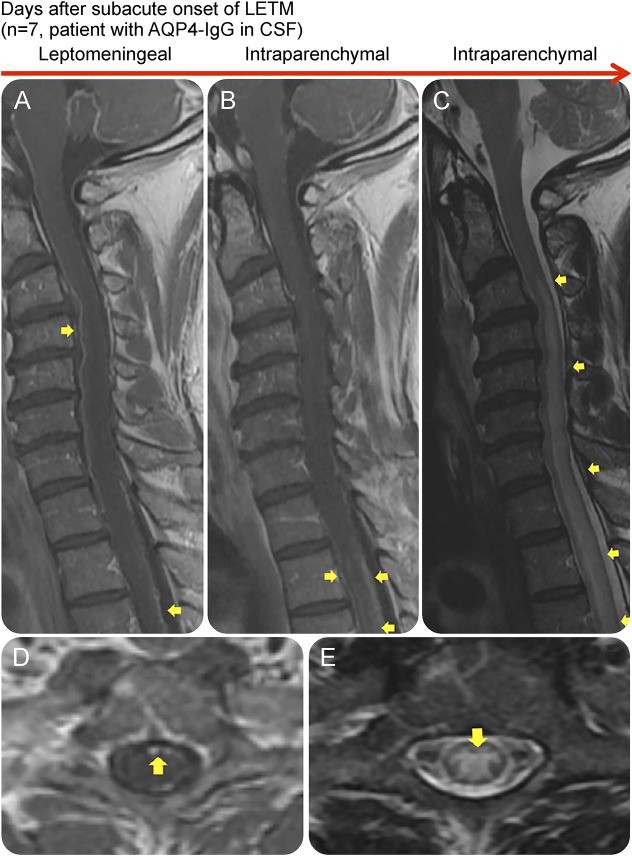
Results: LME was demonstrated on postcontrast T1-weighted and fluid-attenuated inversion recovery images as a sign of leptomeningeal blood-barrier disruption and transient leakage of contrast agent into the subarachnoid space in 11 patients, 6 in the brain and 6 in the spinal cord. The patterns of LME were linear or extensive and were accompanied by periependymal enhancement in 5 cases and intraparenchymal enhancement in all cases. The location of LME in the spinal cord was adjacent to intraparenchymal contrast enhancement with involvement of a median number of 12 (range 5-17) vertebral segments. At the time of LME on MRI, all patients had a clinical attack such as encephalopathy (36%) and/or myelopathy (70%) with median interval between symptom onset and LME of 12 days (range 2-30). LME occurred in association with an initial area postrema attack (44%), signs of systemic infection (33%), or AQP4-IgG in CSF (22%) followed by clinical progression. LME was found at initial clinical presentation in 5 cases and at clinical relapses leading to a diagnosis of NMOSD in 6 cases.
Conclusion: This study suggests that altered leptomeningeal blood barrier may be accompanied by intraparenchymal blood-brain barrier breakdown in patients with AQP4-IgG-positive NMOSD during relapses.
Figures
References
-
- Wingerchuk DM, Lennon VA, Lucchinetti CF, Pittock SJ, Weinshenker BG. The spectrum of neuromyelitis optica. Lancet Neurol 2007;6:805–815. - PubMed
-
- Kim W, Park MS, Lee SH, et al. Characteristic brain magnetic resonance imaging abnormalities in central nervous system aquaporin-4 autoimmunity. Mult Scler 2010;16:1229–1236. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases