

Reflux esophagitis and its role in the pathogenesis of Barrett's metaplasia
- PMID: 28451845
- PMCID: PMC5488728
- DOI: 10.1007/s00535-017-1342-1
Reflux esophagitis and its role in the pathogenesis of Barrett's metaplasia
Abstract
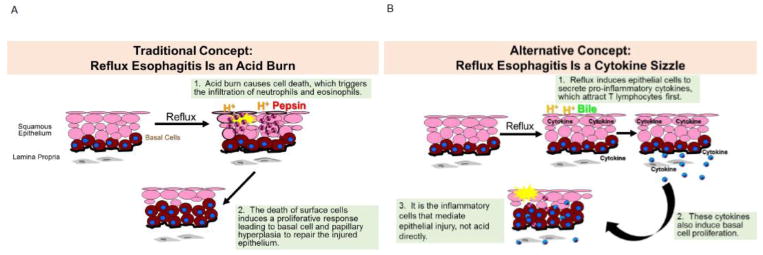
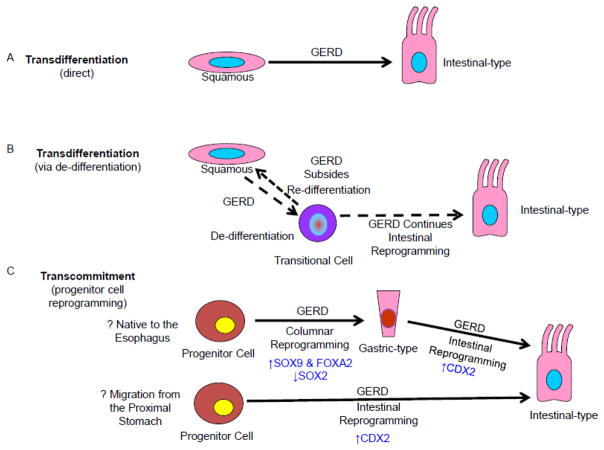
Reflux esophagitis damages the squamous epithelium that normally lines the esophagus, and promotes replacement of the damaged squamous lining by the intestinal metaplasia of Barrett's esophagus, the precursor of esophageal adenocarcinoma. Therefore, to prevent the development of Barrett's metaplasia and esophageal adenocarcinoma, the pathogenesis of reflux esophagitis must be understood. We have reported that reflux esophagitis, both in a rat model and in humans, develops as a cytokine-mediated inflammatory injury (i.e., cytokine sizzle), not as a caustic chemical injury (i.e., acid burn), as traditionally has been assumed. Moreover, reflux induces activation of hypoxia inducible factor (HIF)-2α, which enhances the transcriptional activity of nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) causing increases in pro-inflammatory cytokines and in migration of T lymphocytes, an underlying molecular mechanism for this cytokine-mediated injury. In some individuals, reflux esophagitis heals with Barrett's metaplasia. A number of possibilities exist for the origin of the progenitor cells that give rise to this intestinal metaplasia including those of the esophagus, the proximal stomach, or the bone marrow. However, intestinal cells are not normally found in the esophagus, the stomach, or the bone marrow. Thus, the development of Barrett's intestinal metaplasia must involve some molecular reprogramming of key developmental transcription factors within the progenitor cell, a process termed transcommitment, which may be initiated by the noxious components of the gastric refluxate. This review will highlight recent studies on the pathogenesis of reflux esophagitis and on reflux-related molecular reprogramming of esophageal squamous epithelial cells in the pathogenesis of Barrett's metaplasia.
Keywords: Barrett’s esophagus; Cdx2; Cytokine; NF-κB; Squamous cells.
Conflict of interest statement
Figures

References
-
- Spechler SJ. Carcinogenesis at the gastroesophageal junction: Free radicals at the frontier. Gastroenterology. 2002;122:1518–1520. - PubMed
-
- Spechler SJ, Souza RF. Barrett’s esophagus. The New England journal of medicine. 2014;371:836–845. - PubMed
-
- Iwakiri K, Kinoshita Y, Habu Y, Oshima T, Manabe N, Fujiwara Y, Nagahara A, Kawamura O, Iwakiri R, Ozawa S, Ashida K, Ohara S, Kashiwagi H, Adachi K, Higuchi K, Miwa H, Fujimoto K, Kusano M, Hoshihara Y, Kawano T, Haruma K, Hongo M, Sugano K, Watanabe M, Shimosegawa T. Evidence-based clinical practice guidelines for gastroesophageal reflux disease 2015. Journal of gastroenterology. 2016;51:751–767. - PubMed
-
- Spechler SJ. Clinical practice. Barrett’s esophagus The New England journal of medicine. 2002;346:836–842. - PubMed
-
- Ismail-Beigi F, Horton PF, Pope CE., 2nd Histological consequences of gastroesophageal reflux in man. Gastroenterology. 1970;58:163–174. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
