

Prediction of overall survival in stage II and III colon cancer beyond TNM system: a retrospective, pooled biomarker study
- PMID: 28453697
- PMCID: PMC5406760
- DOI: 10.1093/annonc/mdx052
Prediction of overall survival in stage II and III colon cancer beyond TNM system: a retrospective, pooled biomarker study
Abstract
Background: TNM staging alone does not accurately predict outcome in colon cancer (CC) patients who may be eligible for adjuvant chemotherapy. It is unknown to what extent the molecular markers microsatellite instability (MSI) and mutations in BRAF or KRAS improve prognostic estimation in multivariable models that include detailed clinicopathological annotation.
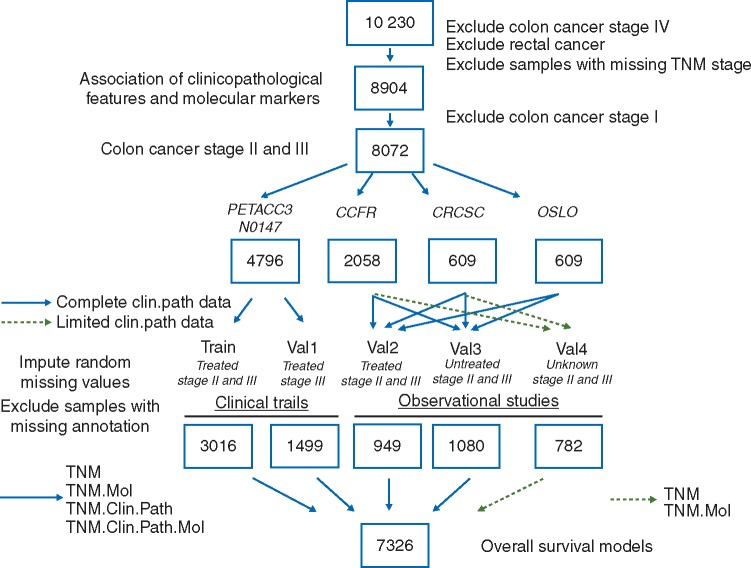
Patients and methods: After imputation of missing at random data, a subset of patients accrued in phase 3 trials with adjuvant chemotherapy (n = 3016)-N0147 (NCT00079274) and PETACC3 (NCT00026273)-was aggregated to construct multivariable Cox models for 5-year overall survival that were subsequently validated internally in the remaining clinical trial samples (n = 1499), and also externally in different population cohorts of chemotherapy-treated (n = 949) or -untreated (n = 1080) CC patients, and an additional series without treatment annotation (n = 782).
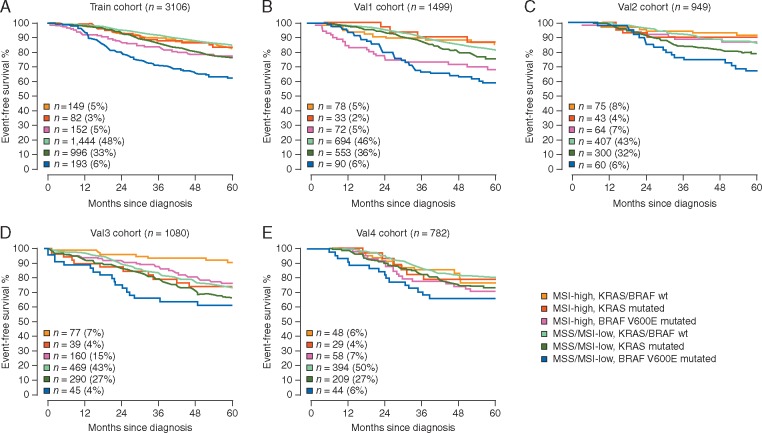
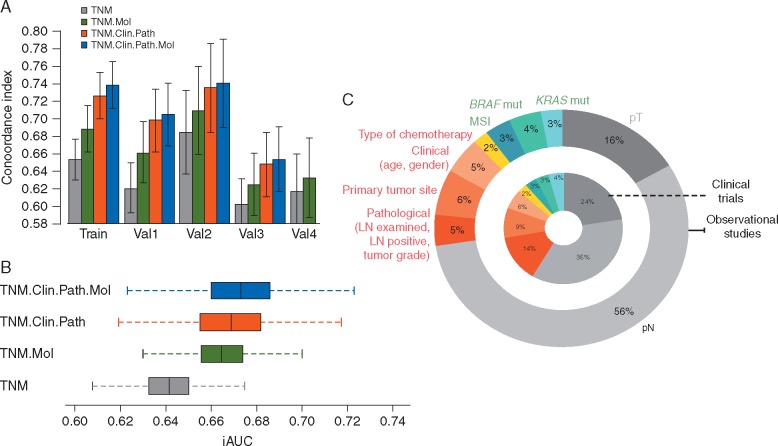
Results: TNM staging, MSI and BRAFV600E mutation status remained independent prognostic factors in multivariable models across clinical trials cohorts and observational studies. Concordance indices increased from 0.61-0.68 in the TNM alone model to 0.63-0.71 in models with added molecular markers, 0.65-0.73 with clinicopathological features and 0.66-0.74 with all covariates. In validation cohorts with complete annotation, the integrated time-dependent AUC rose from 0.64 for the TNM alone model to 0.67 for models that included clinicopathological features, with or without molecular markers. In patient cohorts that received adjuvant chemotherapy, the relative proportion of variance explained (R2) by TNM, clinicopathological features and molecular markers was on an average 65%, 25% and 10%, respectively.
Conclusions: Incorporation of MSI, BRAFV600E and KRAS mutation status to overall survival models with TNM staging improves the ability to precisely prognosticate in stage II and III CC patients, but only modestly increases prediction accuracy in multivariable models that include clinicopathological features, particularly in chemotherapy-treated patients.
Keywords: BRAF mutation; KRAS mutation; colon cancer; microsatellite instability; prognosis.
© The Author 2017. Published by Oxford University Press on behalf of the European Society for Medical Oncology.
Figures
Comment in
-
Including Lynch syndrome in personalized prognostication and follow-up of stage II and III colon cancer.Ann Oncol. 2017 Oct 1;28(10):2620-2621. doi: 10.1093/annonc/mdx292. Ann Oncol. 2017. PMID: 28945832 No abstract available.
-
Reply to the letter to the editor 'Including lynch syndrome in personalized prognostication and follow-up of stage II and III colon cancer' by Sciallero et al.Ann Oncol. 2017 Nov 1;28(11):2889-2890. doi: 10.1093/annonc/mdx415. Ann Oncol. 2017. PMID: 29045507 No abstract available.
-
Is the tumour microenvironment a critical prognostic factor in early-stage colorectal cancer?Ann Oncol. 2019 Oct 1;30(10):1538-1540. doi: 10.1093/annonc/mdz294. Ann Oncol. 2019. PMID: 31504141 Free PMC article. No abstract available.
References
-
- Siegel R, Desantis C, Jemal A.. Colorectal cancer statistics, 2014. CA Cancer J Clin 2014; 64: 104–117. - PubMed
-
- Ferlay J, Steliarova-Foucher E, Lortet-Tieulent J. et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur J Cancer 2013; 49: 1374–1403. - PubMed
-
- National Cancer Institute’s SEER database. http://seer.cancer.gov/ (26 August 2016, date last accessed).
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
