

Incidence of pseudoprogression in low-grade gliomas treated with radiotherapy
- PMID: 28453748
- PMCID: PMC5464441
- DOI: 10.1093/neuonc/now194
Incidence of pseudoprogression in low-grade gliomas treated with radiotherapy
Abstract
Background: As the incidence of pseudo-progressive disease (psPD), or pseudoprogression, in low-grade glioma (LGG) is unknown, we retrospectively investigated this phenomenon in a cohort of LGG patients given radiotherapy (RT).
Methods: All MRI scans and clinical data from patients with histologically proven LGG treated with radiation between 2000 and 2011 were reviewed. PsPD was scored when a new enhancing lesion occurred after RT and subsequently disappeared or remained stable for at least a year without therapy, including dexamethasone.
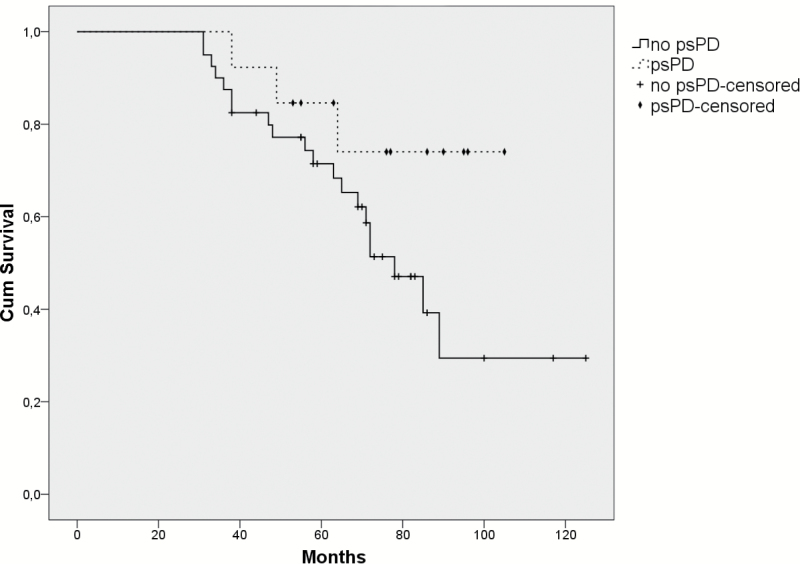
Results: Sixty-three out of 71 patients who received RT for LGG were deemed eligible for evaluation of psPD. The median follow-up was 5 years (range 1‒10 y). PsPD was seen in 13 patients (20.6%). PsPD occurred after a median of 12 months with a range of 3-78 months. The median duration of psPD was 6 months, with a range of 2-26 months and always occurred within the RT high dose fields of at least 45 Gy. The area of the enhancement at the time of psPD was significantly smaller compared with the area of enhancement during "true" progression (median size 54mm2 [range 12-340mm2] vs 270mm2 [range 30-3420mm2], respectively; P = .009).
Conclusions: PsPD occurs frequently in LGG patients receiving RT. This supports the policy to postpone a new line of treatment until progression is evident, especially when patients have small contrast enhancing lesions within the RT field.
Keywords: LGG; glioma; low-grade glioma; pseudoprogression; radiotherapy.
© The Author(s) 2016. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com
Figures



References
-
- van den Bent MJ, Wefel JS, Schiff D, et al. Response assessment in neuro-oncology (a report of the RANO group): assessment of outcome in trials of diffuse low-grade gliomas. Lancet Oncol. 2011;12(6):583–593. - PubMed
-
- Kumthekar P, Raizer J, Singh S. Low-grade glioma. Cancer Treat Res. 2015;163:75–87. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
