

Clinical and patient-reported outcomes of SPARE - a randomised feasibility study of selective bladder preservation versus radical cystectomy
- PMID: 28453896
- PMCID: PMC5655733
- DOI: 10.1111/bju.13900
Clinical and patient-reported outcomes of SPARE - a randomised feasibility study of selective bladder preservation versus radical cystectomy
Abstract
Objectives: To test the feasibility of a randomised trial in muscle-invasive bladder cancer (MIBC) and compare outcomes in patients who receive neoadjuvant chemotherapy followed by radical cystectomy (RC) or selective bladder preservation (SBP), where definitive treatment [RC or radiotherapy (RT)] is determined by response to chemotherapy.
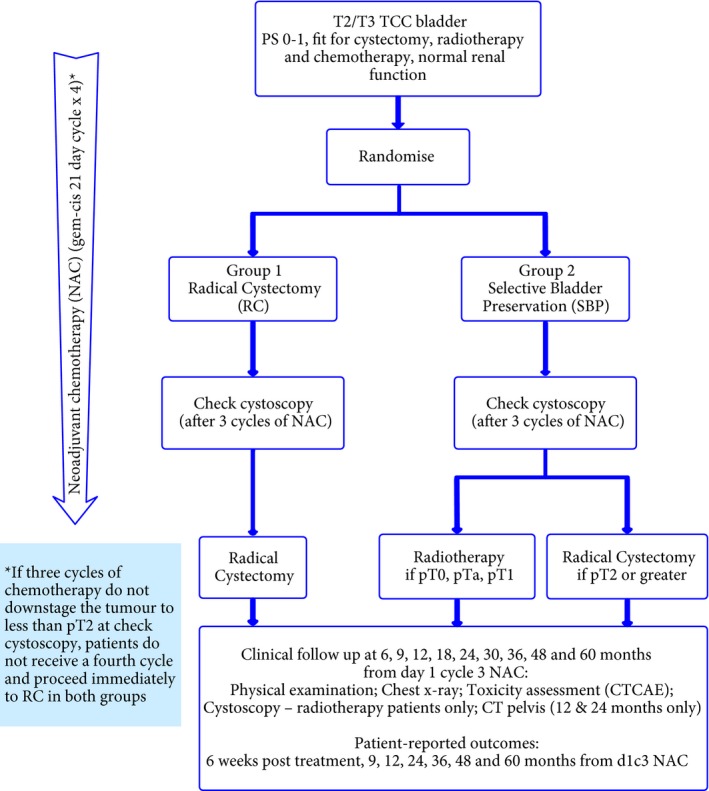
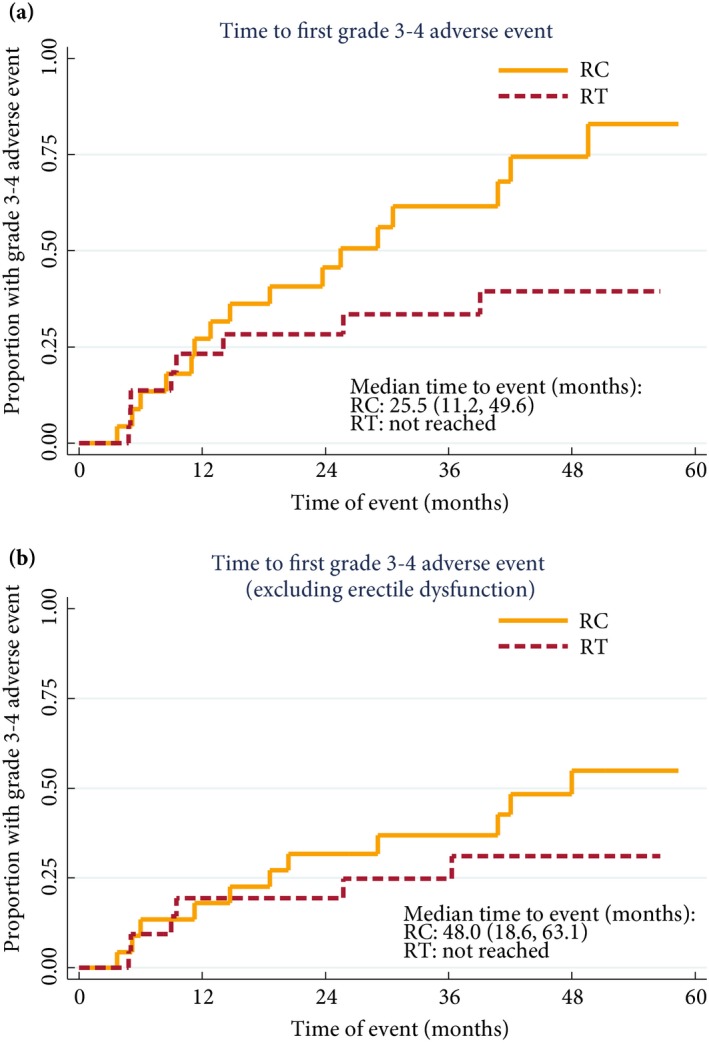
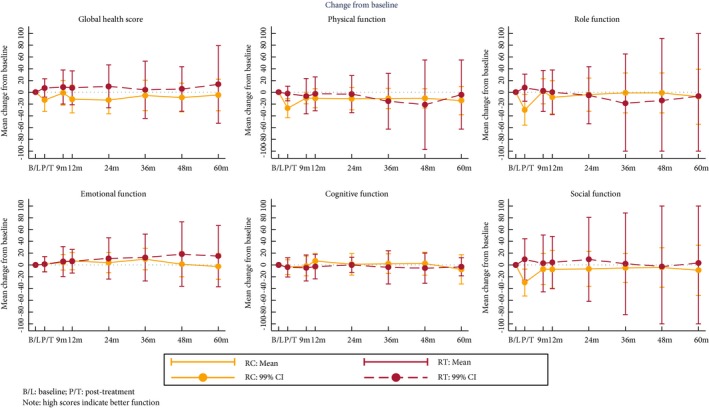
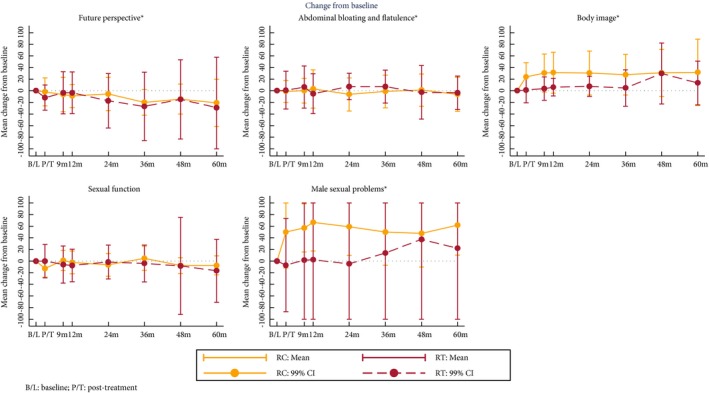
Patients and methods: SPARE is a multicentre randomised controlled trial comparing RC and SBP in patients with MIBC staged T2-3 N0 M0, fit for both treatment strategies and receiving three cycles of neoadjuvant chemotherapy. Patients were randomised between RC and SBP before a cystoscopy after cycle three of neoadjuvant chemotherapy. Patients with ≤T1 residual tumour received a fourth cycle of neoadjuvant chemotherapy in both groups, followed by radical RT in the SBP group and RC in in the RC group; non-responders in both groups proceeded immediately to RC following cycle three. Feasibility study primary endpoints were accrual rate and compliance with assigned treatment strategy. The phase III trial was designed to demonstrate non-inferiority of SBP in terms of overall survival (OS) in patients whose tumours responded to neoadjuvant chemotherapy. Secondary endpoints included patient-reported quality of life, clinician assessed toxicity, loco-regional recurrence-free survival, and rate of salvage RC after SBP.
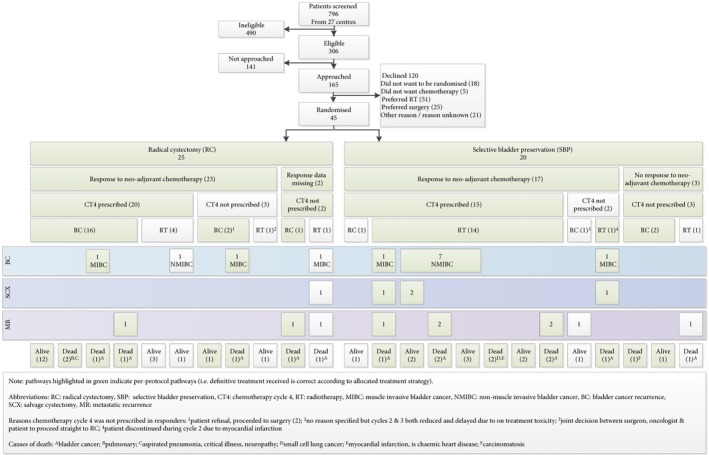
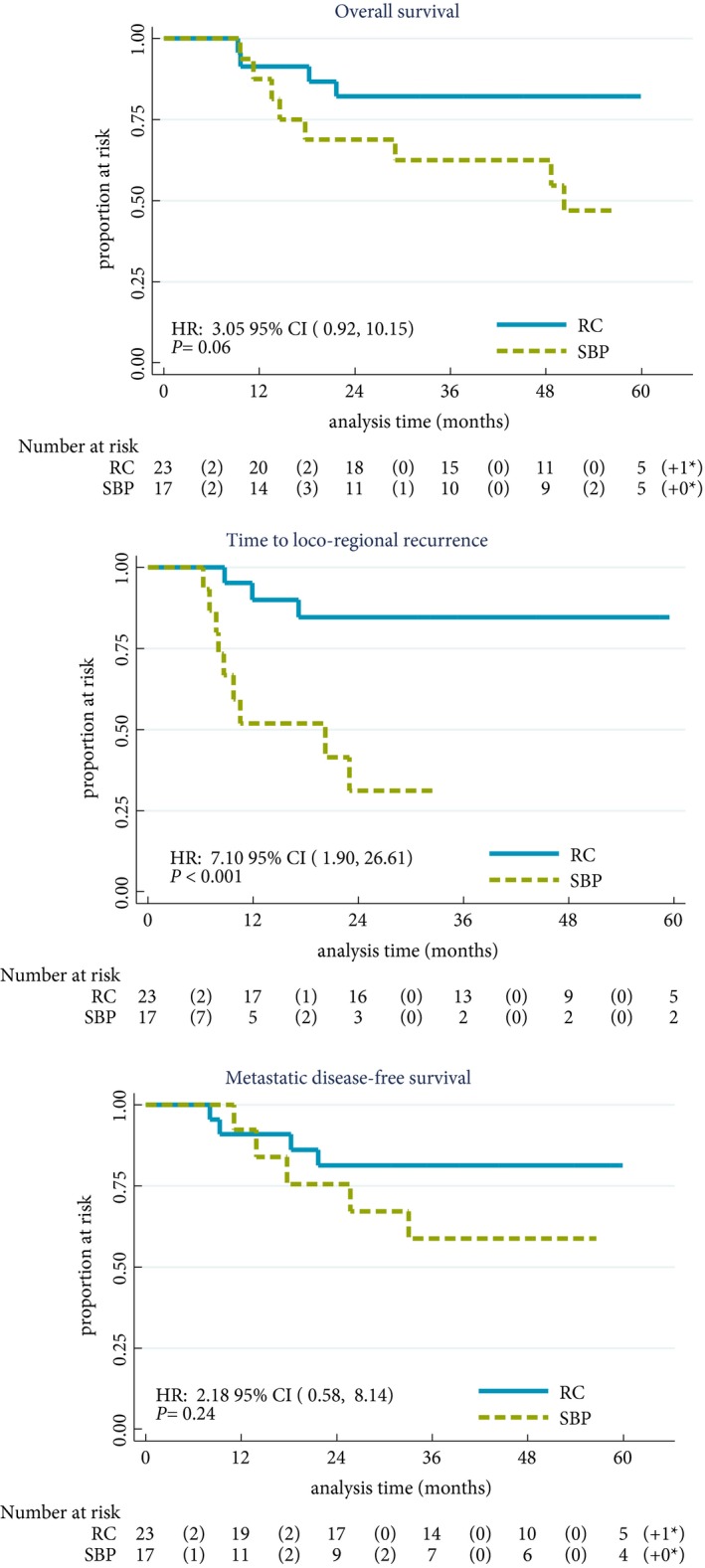
Results: Trial recruitment was challenging and below the predefined target with 45 patients recruited in 30 months (25 RC; 20 SBP). Non-compliance with assigned treatment strategy was frequent, six of the 25 patients (24%) randomised to RC received RT. Long-term bladder preservation rate was 11/15 (73%) in those who received RT per protocol. OS survival was not significantly different between groups.
Conclusions: Randomising patients with MIBC between RC and SBP based on response to neoadjuvant chemotherapy was not feasible in the UK health system. Strong clinician and patient preferences for treatments impacted willingness to undergo randomisation and acceptance of treatment allocation. Due to the few participants, firm conclusions about disease and toxicity outcomes cannot be drawn.
Keywords: #BladderCancer; #blcsm; muscle-invasive bladder cancer; radical cystectomy; radiotherapy; randomised controlled trial; selective bladder preservation.
© 2017 The Authors. BJU International published by John Wiley & Sons Ltd on behalf of BJU International.
Figures
Comment in
-
Should we care more about SPARE?BJU Int. 2017 Nov;120(5):605-606. doi: 10.1111/bju.13953. BJU Int. 2017. PMID: 29035018 No abstract available.
References
-
- Cookson MS. The surgical management of muscle invasive bladder cancer: a contemporary review. Semin Radiat Oncol 2005; 15: 10–8 - PubMed
-
- Hautmann RE, de Petriconi R, Gottfried HW, Kleinschmidt K, Mattes R, Paiss T. The ileal neobladder: complications and functional results in 363 patients after 11 years of followup. J Urol 1999; 161: 422–8 - PubMed
-
- Fosså SD, Waehre H, Aass N, Jacobsen AB, Olsen DR, Ous S. Bladder cancer definitive radiation therapy of muscle‐lnvasive bladder cancer – a retrospective analysis of 317 patients. Cancer 1993; 72: 3036–43 - PubMed
-
- Shipley WU, Zietman AL, Kaufman DS, Coen JJ, Sandler HM. Selective bladder preservation by trimodality therapy for patients with muscularis propria‐invasive bladder cancer and who are cystectomy candidates – the Massachusetts General Hospital and Radiation Therapy Oncology Group experiences. Semin Radiat Oncol 2005; 15: 36–41 - PubMed
-
- Ramani VA, Maddineni SB, Grey BR, Clarke NW. Differential complication rates following radical cystectomy in the irradiated and nonirradiated pelvis. Eur Urol 2010; 57: 1058–63 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
