

Dyslipidemia and reference values for fasting plasma lipid concentrations in Danish/North-European White children and adolescents
- PMID: 28454530
- PMCID: PMC5410076
- DOI: 10.1186/s12887-017-0868-y
Dyslipidemia and reference values for fasting plasma lipid concentrations in Danish/North-European White children and adolescents
Abstract
Background: Dyslipidemia is reported in 27 - 43% of children and adolescents with overweight/obesity and tracks into adulthood, increasing the risk of cardiovascular morbidity. Cut-off values for fasting plasma lipid concentrations are typically set at fixed levels throughout childhood. The objective of this cross-sectional study was to generate fasting plasma lipid references for a Danish/North-European White population-based cohort of children and adolescents, and investigate the prevalence of dyslipidemia in this cohort as well as in a cohort with overweight/obesity.
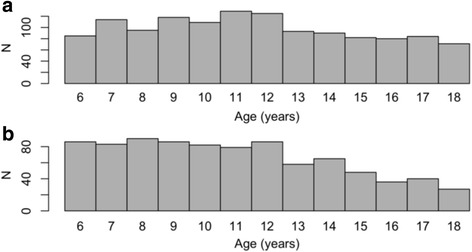
Methods: A population-based cohort of 2141 (1275 girls) children and adolescents aged 6 - 19 (median 11.5) years was recruited from 11 municipalities in Denmark. Additionally, a cohort of children and adolescents of 1421 (774 girls) with overweight/obesity aged 6 - 19 years (median 11.8) was recruited for the study. Height, weight, and fasting plasma lipid concentrations were measured on all participants. Smoothed reference curves and percentiles were generated using the Generalized Additive Models for Location Scale and Shape package in the statistical software R.
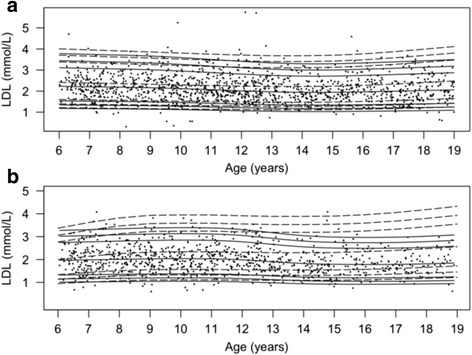
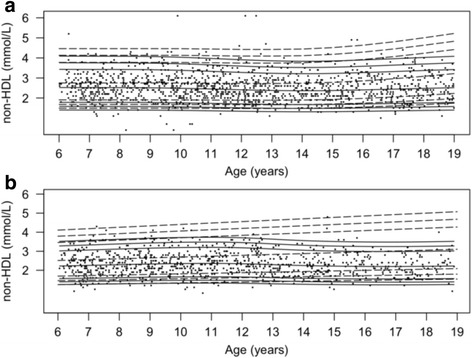
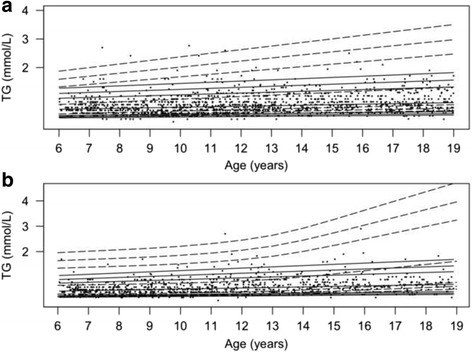
Results: In the population-based cohort, plasma concentrations of total cholesterol (TC) (P < 0.05), low-density lipoprotein cholesterol (LDL) (P < 0.005), and high-density lipoprotein cholesterol (HDL) (P < 0.005) were higher in the youngest compared to the oldest tertile. Fasting plasma levels of triglycerides (TG) (P < 0.005) increased with age in both sexes. In boys, non-HDL was lower in the oldest compared to the youngest tertile (P < 0.0005). Concentrations of TC, LDL, non-HDL, and TG were higher (P < 0.05), and HDL lower (P < 0.05) in the cohort with overweight/obesity in both sexes and for all ages except for TC in the youngest girls. The overall prevalence of dyslipidemia was 6.4% in the population-based cohort and 28.0% in the cohort with overweight/obesity. The odds ratio for exhibiting dyslipidemia in the cohort with overweight/obesity compared with the population-based cohort was 6.2 (95% CI: 4.9 - 8.1, P < 2*10-16).
Conclusion: Fasting plasma lipid concentrations change during childhood and adolescence and differ with sex and age. Children and adolescents with obesity have increased concentrations of circulating lipids and exhibit an increased prevalence of dyslipidemia.
Trial registration: The study is part of The Danish Childhood Obesity Biobank; ClinicalTrials.gov ID-no.: NCT00928473 retrospectively registered on June 25th 2009.
Keywords: Adolescent; Child; Dyslipidemias; Lipids; Obesity; Reference values.
Figures


References
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2013;380(9859):2095–2128. doi: 10.1016/S0140-6736(12)61728-0. - DOI - PMC - PubMed
-
- Perk J, De Backer G, Gohlke H, Graham I, Reiner Z, Verschuren M, et al. European Guidelines on cardiovascular disease prevention in clinical practice (version 2012). The Fifth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice (constituted by representatives of nine societies and by invited experts) Eur Heart J. 2012;33(13):1635–1701. doi: 10.1093/eurheartj/ehs092. - DOI - PubMed
-
- Nomikos T, Panagiotakos D, Georgousopoulou E, Metaxa V, Chrysohoou C, Skoumas I, et al. Hierarchical modelling of blood lipids’ profile and 10-year (2002-2012) all cause mortality and incidence of cardiovascular disease: the ATTICA study. Lipids Health Dis. 2015;14:108. doi: 10.1186/s12944-015-0101-7. - DOI - PMC - PubMed
-
- Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children And Adolescents Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents: Summary Report. Pediatrics. 2011;128(Supplement 5):S213–S256. doi: 10.1542/peds.2009-2107C. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
