

Protective intraoperative ventilation with higher versus lower levels of positive end-expiratory pressure in obese patients (PROBESE): study protocol for a randomized controlled trial
- PMID: 28454590
- PMCID: PMC5410049
- DOI: 10.1186/s13063-017-1929-0
Protective intraoperative ventilation with higher versus lower levels of positive end-expiratory pressure in obese patients (PROBESE): study protocol for a randomized controlled trial
Erratum in
-
Erratum to Protective intraoperative ventilation with higher versus lower levels of positive end-expiratory pressure in obese patients (PROBESE): study protocol for a randomized controlled trial.Trials. 2017 Jun 1;18(1):247. doi: 10.1186/s13063-017-1987-3. Trials. 2017. PMID: 28571581 Free PMC article. No abstract available.
Abstract
Background: Postoperative pulmonary complications (PPCs) increase the morbidity and mortality of surgery in obese patients. High levels of positive end-expiratory pressure (PEEP) with lung recruitment maneuvers may improve intraoperative respiratory function, but they can also compromise hemodynamics, and the effects on PPCs are uncertain. We hypothesized that intraoperative mechanical ventilation using high PEEP with periodic recruitment maneuvers, as compared with low PEEP without recruitment maneuvers, prevents PPCs in obese patients.
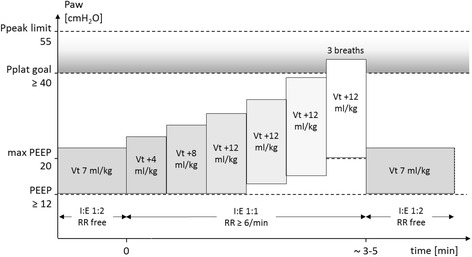
Methods/design: The PRotective Ventilation with Higher versus Lower PEEP during General Anesthesia for Surgery in OBESE Patients (PROBESE) study is a multicenter, two-arm, international randomized controlled trial. In total, 2013 obese patients with body mass index ≥35 kg/m2 scheduled for at least 2 h of surgery under general anesthesia and at intermediate to high risk for PPCs will be included. Patients are ventilated intraoperatively with a low tidal volume of 7 ml/kg (predicted body weight) and randomly assigned to PEEP of 12 cmH2O with lung recruitment maneuvers (high PEEP) or PEEP of 4 cmH2O without recruitment maneuvers (low PEEP). The occurrence of PPCs will be recorded as collapsed composite of single adverse pulmonary events and represents the primary endpoint.
Discussion: To our knowledge, the PROBESE trial is the first multicenter, international randomized controlled trial to compare the effects of two different levels of intraoperative PEEP during protective low tidal volume ventilation on PPCs in obese patients. The results of the PROBESE trial will support anesthesiologists in their decision to choose a certain PEEP level during general anesthesia for surgery in obese patients in an attempt to prevent PPCs.
Trial registration: ClinicalTrials.gov identifier: NCT02148692. Registered on 23 May 2014; last updated 7 June 2016.
Keywords: Mechanical ventilation; Obesity; Positive end-expiratory pressure; Postoperative pulmonary complication; Recruitment maneuver.
Figures

References
-
- Serpa Neto A, Hemmes SN, Barbas CS, Beiderlinden M, Fernandez-Bustamante A, Futier E, et al. Incidence of mortality and morbidity related to postoperative lung injury in patients who have undergone abdominal or thoracic surgery: a systematic review and meta-analysis. Lancet Respir Med. 2014;2:1007–15. doi: 10.1016/S2213-2600(14)70228-0. - DOI - PubMed
-
- Canet J, Sabaté S, Mazo V, Gallart L, de Abreu MG, Belda J, et al. Development and validation of a score to predict postoperative respiratory failure in a multicentre European cohort: a prospective, observational study. Eur J Anaesthesiol. 2015;32:458–70. doi: 10.1097/EJA.0000000000000223. - DOI - PubMed
-
- Guldner A, Kiss T, Serpa Neto A, Hemmes SN, Canet J, Spieth PM, et al. Intraoperative protective mechanical ventilation for prevention of postoperative pulmonary complications: a comprehensive review of the role of tidal volume, positive end-expiratory pressure, and lung recruitment maneuvers. Anesthesiology. 2015;123:692–713. doi: 10.1097/ALN.0000000000000754. - DOI - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
