

Opioids Cause Central and Complex Sleep Apnea in Humans and Reversal With Discontinuation: A Plea for Detoxification
- PMID: 28454596
- PMCID: PMC5443744
- DOI: 10.5664/jcsm.6628
Opioids Cause Central and Complex Sleep Apnea in Humans and Reversal With Discontinuation: A Plea for Detoxification
Abstract
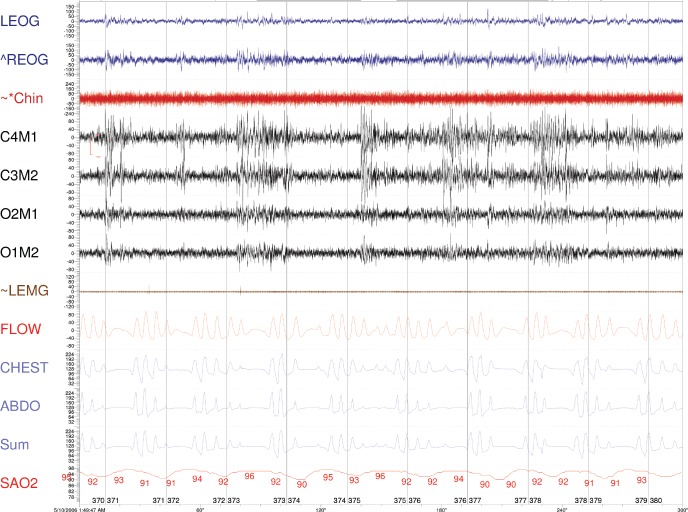
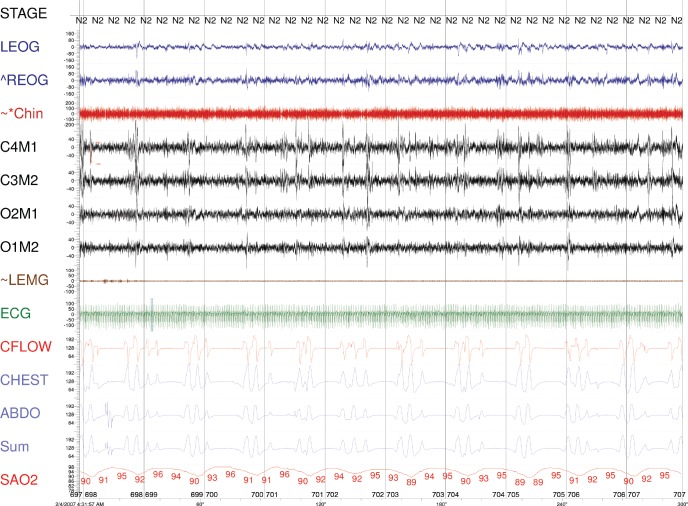
Central sleep apnea (CSA) and continuous positive airway pressure (CPAP) emergent CSA are common in patients for whom opioids have been prescribed for chronic pain management. It is not known if opioids are the potential cause of CSA. We report the case of a patient who underwent multiple full nights of polysomnography testing while on opioids, off opioids, and with various positive airway pressure devices. While on opioids, the patient had severe CSA that persisted during both CPAP and bilevel titration but was eliminated with adaptive servoventilation therapy. Some time later, opioid use was discontinued by the patient. Repeat polysomnography showed resolution of the sleep-disordered breathing. Later-while the patient was still off opioids-she had gained weight and become symptomatic; polysomnography showed obstructive sleep apnea without CSA. This time, therapy with CPAP showed elimination of sleep apnea without emergent CSA. These data collectively indicate that opioids were the cause of CSA as well as emergent CSA.
Keywords: adaptive servoventilation; central sleep apnea.
© 2017 American Academy of Sleep Medicine
Figures
References
-
- Dowell D, Haegerich TM, Chou R. CDC guideline for prescribing opioids for chronic pain - United States, 2016. MMWR Recomm Rep. 2016;65(1):1–49. - PubMed
-
- Javaheri S, Randerath WJ. Opioid-induced central sleep apnea: mechanisms and therapies. Sleep Med Clin. 2014;9(1):49–56.
-
- Farney RJ, McDonald AM, Boyle KM, et al. Sleep disordered breathing in patients receiving therapy with buprenorphine/naloxone. Eur Respir J. 2013;42(2):394–403. - PubMed
-
- Guilleminault C, Cao M, Yue HJ, Chawla P. Obstructive sleep apnea and chronic opioid use. Lung. 2010;188(6):459–468. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
