

Weight Loss and Improvement in Comorbidity: Differences at 5%, 10%, 15%, and Over
- PMID: 28455679
- PMCID: PMC5497590
- DOI: 10.1007/s13679-017-0262-y
Weight Loss and Improvement in Comorbidity: Differences at 5%, 10%, 15%, and Over
Abstract
Purpose of review: One begins to see improvement in glycemic measures and triglycerides with small amounts of weight loss, but with greater levels of weight loss there is even greater improvement. In fact, the relationship between weight loss and glycemia is one that is very close.
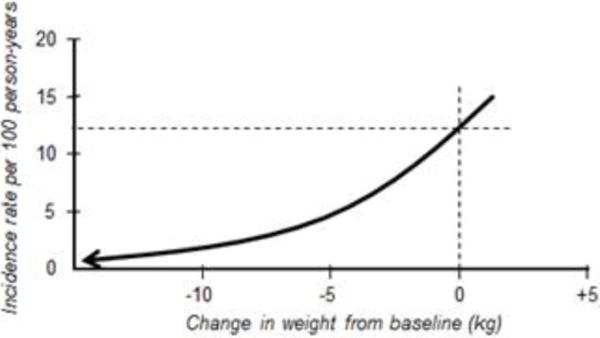
Recent findings: This is fortunate for diabetes prevention; it takes only small amounts of weight loss to prevent progression to type 2 diabetes from impaired glucose tolerance, and after the 10 kg of weight loss, one cannot demonstrate much additional improvement in risk reduction. Modest weight loss (5 to 10%) is also associated with improvement in systolic and diastolic blood pressure and HDL cholesterol. With all these risk factors, more weight loss produces more improvement. Further, for patients with higher BMI levels (>40 kg/m2), the ability to lose the same proportion of weight with lifestyle intervention is equal to that of those with lower BMI levels, and there is equal benefit in terms of risk factor improvement with modest weight loss. For some comorbid conditions, more weight loss is needed-10 to 15%-to translate into clinical improvement. This is true with obstructive sleep apnea and non-alcoholic steatotic hepatitis. There is a graded improvement in improvements in measures of quality of life, depression, mobility, sexual dysfunction, and urinary stress incontinence, whereby improvements are demonstrable with modest weight loss (5-10%) and with further weight loss there are further improvements. For polycystic ovarian syndrome and infertility, modest weight loss (beginning at 2-5%) can bring improvements in menstrual irregularities and fertility. Moderate weight loss (5-10%) has been shown to be associated with reduced health care costs. Reduction in mortality may take more than 10% weight loss, although definitive studies have not been done to demonstrate that weight loss per se is associated with mortality reduction. Clinicians in medical weight management should bear in mind that the target should be health improvement rather than a number on the scale. The individual patient's targeted health goal should be assessed for response rather than a prescribed percentage weight loss.
Keywords: Dysglycemia; Dyslipidemia; Hypertension; Infertility; Non-alcoholic fatty liver disease; Obesity; Obesity comorbidity; Obstructive sleep apnea; Polycystic ovarian syndrome; Type 2 diabetes; Weight loss; Weight loss and comorbidity improvement; Weight management.
Conflict of interest statement
Donna H. Ryana and Sarah Ryan Yockey declare they have no conflict of interest.
Figures
References
-
- Williamson DA, Bray GA, Ryan DH. Is 5% weight loss a satisfactory criterion to define clinically significant weight loss? Obesity (Silver Spring) 2015 Dec;23(12):2319–20. - PubMed
-
- Jensen MD, Ryan DH, Donato KA, et al. Guidelines 2013 for managing overweight and obesity in adults. Obesity. 2014;22:S1–S410. These guidelines are based on a systematic evidence review around 5 critical questions (benefits of weight loss, risks of excess body weight, best diet for weight loss, weight loss with comprehensive lifestyle intervention and role of bariatric surgery). - PubMed
-
- U.S. Department of Health and Human Services Food and Drug Administration. Center for Drug Evaluation and Research (CDEER) Guidance for Industry Developing products for Weight Management. Draft Guidance. 2007 Feb; Revision 1. http://www.fda.gov/downloads/Drugs/GuidanceComplianceRegulatoryInformati... Accessed 1/7/2017.
-
- Messier RP, Gutekunst DJ, Davis C, DeVita P. ARTHRITIS & RHEUMATISM. 2005;52(7):2026–32. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
