

Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial
- PMID: 28456509
- PMCID: PMC5446563
- DOI: 10.1016/S0140-6736(17)30638-4
Effect of early tranexamic acid administration on mortality, hysterectomy, and other morbidities in women with post-partum haemorrhage (WOMAN): an international, randomised, double-blind, placebo-controlled trial
Erratum in
-
Department of Error.Lancet. 2017 May 27;389(10084):2104. doi: 10.1016/S0140-6736(17)31220-5. Epub 2017 May 5. Lancet. 2017. PMID: 28483296 Free PMC article. No abstract available.
Abstract
Background: Post-partum haemorrhage is the leading cause of maternal death worldwide. Early administration of tranexamic acid reduces deaths due to bleeding in trauma patients. We aimed to assess the effects of early administration of tranexamic acid on death, hysterectomy, and other relevant outcomes in women with post-partum haemorrhage.
Methods: In this randomised, double-blind, placebo-controlled trial, we recruited women aged 16 years and older with a clinical diagnosis of post-partum haemorrhage after a vaginal birth or caesarean section from 193 hospitals in 21 countries. We randomly assigned women to receive either 1 g intravenous tranexamic acid or matching placebo in addition to usual care. If bleeding continued after 30 min, or stopped and restarted within 24 h of the first dose, a second dose of 1 g of tranexamic acid or placebo could be given. Patients were assigned by selection of a numbered treatment pack from a box containing eight numbered packs that were identical apart from the pack number. Participants, care givers, and those assessing outcomes were masked to allocation. We originally planned to enrol 15 000 women with a composite primary endpoint of death from all-causes or hysterectomy within 42 days of giving birth. However, during the trial it became apparent that the decision to conduct a hysterectomy was often made at the same time as randomisation. Although tranexamic acid could influence the risk of death in these cases, it could not affect the risk of hysterectomy. We therefore increased the sample size from 15 000 to 20 000 women in order to estimate the effect of tranexamic acid on the risk of death from post-partum haemorrhage. All analyses were done on an intention-to-treat basis. This trial is registered with ISRCTN76912190 (Dec 8, 2008); ClinicalTrials.gov, number NCT00872469; and PACTR201007000192283.
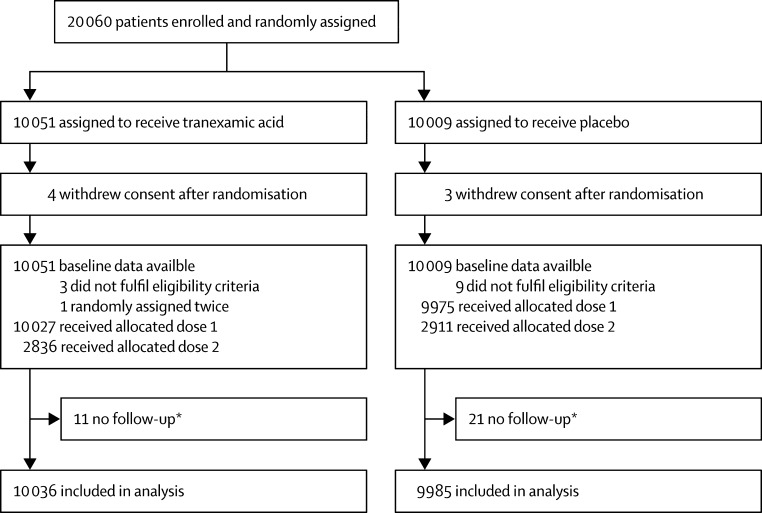
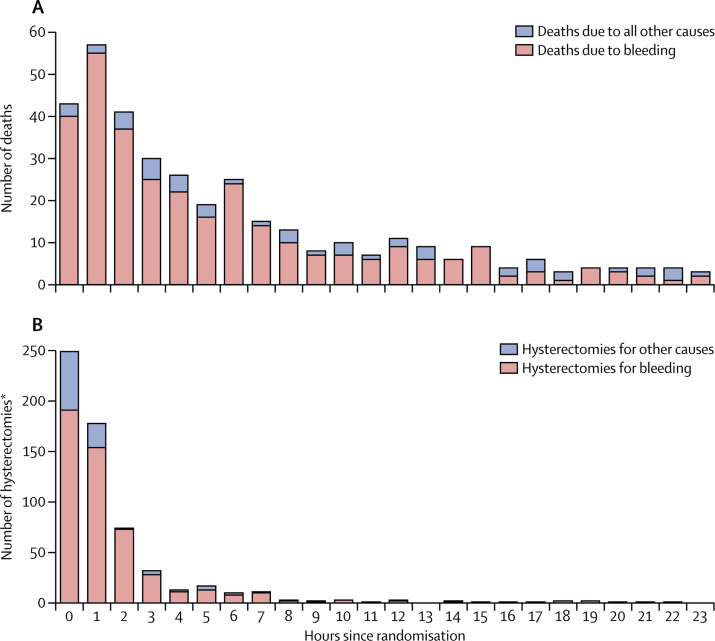
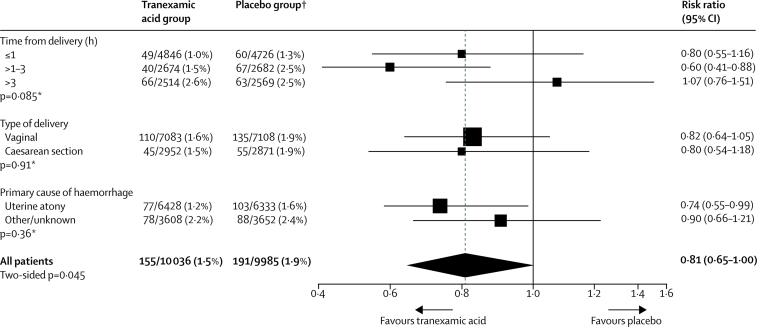
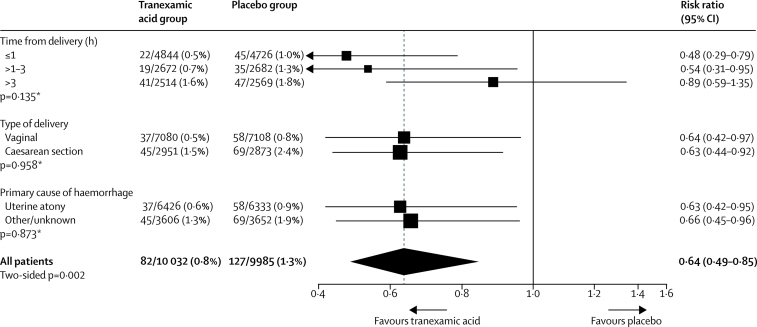
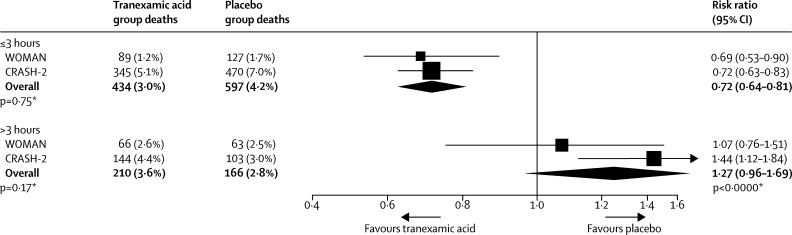
Findings: Between March, 2010, and April, 2016, 20 060 women were enrolled and randomly assigned to receive tranexamic acid (n=10 051) or placebo (n=10 009), of whom 10 036 and 9985, respectively, were included in the analysis. Death due to bleeding was significantly reduced in women given tranexamic acid (155 [1·5%] of 10 036 patients vs 191 [1·9%] of 9985 in the placebo group, risk ratio [RR] 0·81, 95% CI 0·65-1·00; p=0·045), especially in women given treatment within 3 h of giving birth (89 [1·2%] in the tranexamic acid group vs 127 [1·7%] in the placebo group, RR 0·69, 95% CI 0·52-0·91; p=0·008). All other causes of death did not differ significantly by group. Hysterectomy was not reduced with tranexamic acid (358 [3·6%] patients in the tranexamic acid group vs 351 [3·5%] in the placebo group, RR 1·02, 95% CI 0·88-1·07; p=0·84). The composite primary endpoint of death from all causes or hysterectomy was not reduced with tranexamic acid (534 [5·3%] deaths or hysterectomies in the tranexamic acid group vs 546 [5·5%] in the placebo group, RR 0·97, 95% CI 0·87-1·09; p=0·65). Adverse events (including thromboembolic events) did not differ significantly in the tranexamic acid versus placebo group.
Interpretation: Tranexamic acid reduces death due to bleeding in women with post-partum haemorrhage with no adverse effects. When used as a treatment for postpartum haemorrhage, tranexamic acid should be given as soon as possible after bleeding onset.
Funding: London School of Hygiene & Tropical Medicine, Pfizer, UK Department of Health, Wellcome Trust, and Bill & Melinda Gates Foundation.
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
WOMAN: reducing maternal deaths with tranexamic acid.Lancet. 2017 May 27;389(10084):2081. doi: 10.1016/S0140-6736(17)31111-X. Epub 2017 Apr 26. Lancet. 2017. PMID: 28456507 No abstract available.
-
Administration of tranexamic acid to reduce maternal mortality related to postpartum haemorrhage: comments on the WOMAN trial.Int J Obstet Anesth. 2018 Feb;33:89-90. doi: 10.1016/j.ijoa.2017.07.010. Epub 2017 Jul 25. Int J Obstet Anesth. 2018. PMID: 28899732 No abstract available.
-
The expanding role of tranexamic acid in the management of obstetric hemorrhage.J Thorac Dis. 2017 Aug;9(8):2251-2254. doi: 10.21037/jtd.2017.07.19. J Thorac Dis. 2017. PMID: 28932517 Free PMC article. No abstract available.
-
Tranexamic acid for post-partum haemorrhage in the WOMAN trial.Lancet. 2017 Sep 30;390(10102):1581-1582. doi: 10.1016/S0140-6736(17)31947-5. Epub 2017 Sep 28. Lancet. 2017. PMID: 28980953 No abstract available.
-
Tranexamic acid for post-partum haemorrhage in the WOMAN trial.Lancet. 2017 Sep 30;390(10102):1582. doi: 10.1016/S0140-6736(17)31946-3. Epub 2017 Sep 28. Lancet. 2017. PMID: 28980954 No abstract available.
-
Tranexamic acid for post-partum haemorrhage in the WOMAN trial.Lancet. 2017 Sep 30;390(10102):1582-1583. doi: 10.1016/S0140-6736(17)31956-6. Epub 2017 Sep 28. Lancet. 2017. PMID: 28980955 No abstract available.
-
Tranexamic acid for post-partum haemorrhage in the WOMAN trial.Lancet. 2017 Sep 30;390(10102):1583-1584. doi: 10.1016/S0140-6736(17)31949-9. Epub 2017 Sep 28. Lancet. 2017. PMID: 28980956 No abstract available.
-
Tranexamic acid for post-partum haemorrhage in the WOMAN trial.Lancet. 2017 Sep 30;390(10102):1583. doi: 10.1016/S0140-6736(17)32408-X. Epub 2017 Sep 28. Lancet. 2017. PMID: 28980957 No abstract available.
-
Gerinnung.Med Klin Intensivmed Notfmed. 2018 Nov;113(8):612-613. doi: 10.1007/s00063-018-0463-5. Med Klin Intensivmed Notfmed. 2018. PMID: 30402663 German. No abstract available.
References
-
- WHO . WHO recommendations for the prevention and treatment of postpartum haemorrhage. World Health Organisation; Geneva: 2012. - PubMed
-
- Carroli G, Cuesta C, Abalos E, Gulmezoglu AM. Epidemiology of postpartum haemorrhage: a systematic review. Best Pract Res Clin Obstet Gynaecol. 2008;22:999–1012. - PubMed
-
- WHO, UNFPA and The World Bank . Trends in maternal mortality: 1990 to 2010 - WHO. UNICEF, UNFPA and The World Bank estimates; 2012.
-
- Ronsmans C, Graham WJ, LMSSS Group Maternal mortality: who, when, where, and why. Lancet. 2006;368:1189–1200. - PubMed
-
- Say L, Chou D, Gemmill A. Global causes of maternal death: a WHO systematic analysis. Lancet Glob Health. 2014;2:e323–e333. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
