

Adenoma surveillance and colorectal cancer incidence: a retrospective, multicentre, cohort study
- PMID: 28457708
- PMCID: PMC5461371
- DOI: 10.1016/S1470-2045(17)30187-0
Adenoma surveillance and colorectal cancer incidence: a retrospective, multicentre, cohort study
Abstract
Background: Removal of adenomas reduces colorectal cancer incidence and mortality; however, the benefit of surveillance colonoscopy on colorectal cancer risk remains unclear. We examined heterogeneity in colorectal cancer incidence in intermediate-risk patients and the effect of surveillance on colorectal cancer incidence.
Methods: We did this retrospective, multicentre, cohort study using routine lower gastrointestinal endoscopy and pathology data from patients who, after baseline colonoscopy and polypectomy, were diagnosed with intermediate-risk adenomas mostly (>99%) between Jan 1, 1990, and Dec 31, 2010, at 17 hospitals in the UK. These patients are currently offered surveillance colonoscopy at intervals of 3 years. Patients were followed up through to Dec 31, 2014.We assessed the effect of surveillance on colorectal cancer incidence using Cox regression with adjustment for patient, procedural, and polyp characteristics. We defined lower-risk and higher-risk subgroups on the basis of polyp and procedural characteristics identified as colorectal cancer risk factors. We estimated colorectal cancer incidence and standardised incidence ratios (SIRs) using as standard the general population of England in 2007. This trial is registered, number ISRCTN15213649.
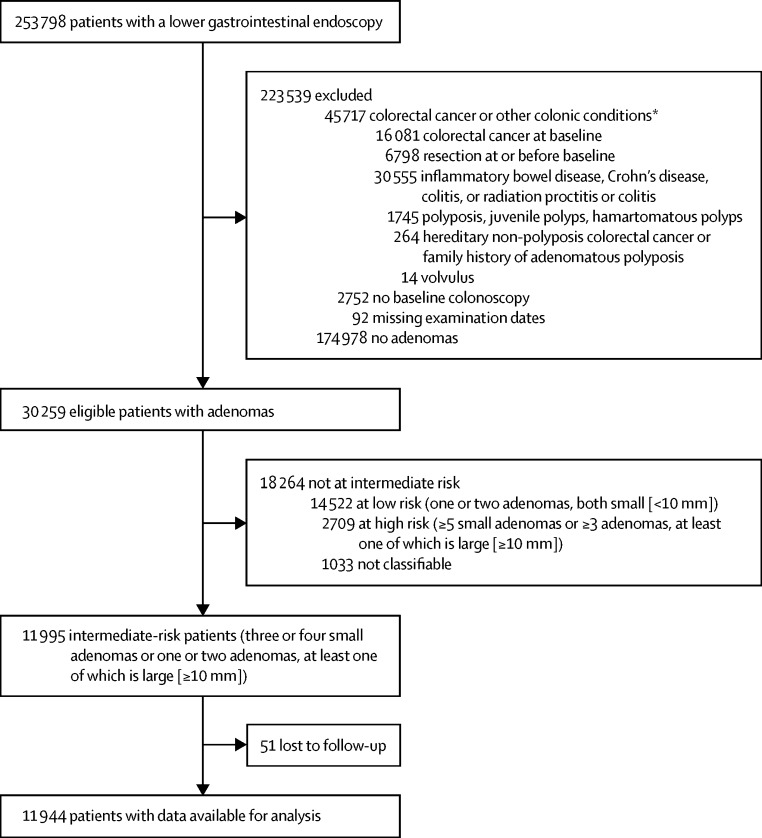
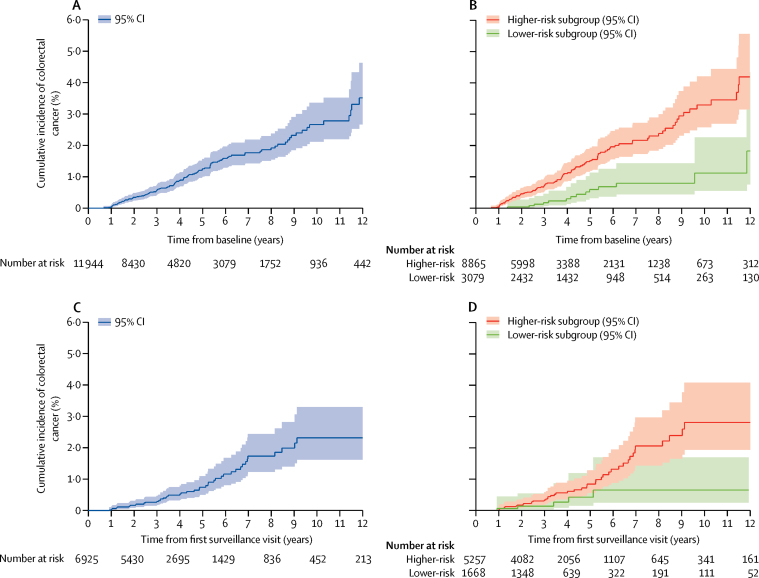
Findings: 253 798 patients who underwent colonic endoscopy were identified, of whom 11 944 with intermediate-risk adenomas were included in this analysis. After a median follow-up of 7·9 years (IQR 5·6-11·1), 210 colorectal cancers were diagnosed. 5019 (42%) patients did not attend surveillance and 6925 (58%) attended one or more surveillance visits. Compared to no surveillance, one or two surveillance visits were associated with a significant reduction in colorectal cancer incidence rate (adjusted hazard ratio 0·57, 95% CI 0·40-0·80 for one visit; 0·51, 0·31-0·84 for two visits). Without surveillance, colorectal cancer incidence in patients with a suboptimal quality colonoscopy, proximal polyps, or a high-grade or large adenoma (≥20 mm) at baseline (8865 [74%] patients) was significantly higher than in the general population (SIR 1·30, 95% CI 1·06-1·57). By contrast, in patients without these features, colorectal cancer incidence was lower than that of the general population (SIR 0·51, 95% CI 0·29-0·84).
Interpretation: Colonoscopy surveillance benefits most patients with intermediate-risk adenomas. However, some patients are already at low risk after baseline colonoscopy and the value of surveillance for them is unclear.
Funding: National Institute for Health Research Health Technology Assessment, Cancer Research UK.
Copyright © 2017 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Can post-polypectomy surveillance be less intensive?Lancet Oncol. 2017 Jun;18(6):707-709. doi: 10.1016/S1470-2045(17)30305-4. Epub 2017 Apr 28. Lancet Oncol. 2017. PMID: 28457710 No abstract available.
-
Colorectal adenomas, surveillance, and cancer.Lancet Oncol. 2017 Aug;18(8):e427. doi: 10.1016/S1470-2045(17)30473-4. Epub 2017 Jul 26. Lancet Oncol. 2017. PMID: 28759374 No abstract available.
-
Colorectal adenomas, surveillance, and cancer - Authors' reply.Lancet Oncol. 2017 Aug;18(8):e428. doi: 10.1016/S1470-2045(17)30532-6. Epub 2017 Jul 26. Lancet Oncol. 2017. PMID: 28759375 No abstract available.
References
-
- Atkin WS, Edwards R, Kralj-Hans I. Once-only flexible sigmoidoscopy screening in prevention of colorectal cancer: a multicentre randomised controlled trial. Lancet. 2010;375:1624–1633. - PubMed
-
- Segnan N, Armaroli P, Bonelli L. Once-only sigmoidoscopy in colorectal cancer screening: follow-up findings of the italian randomized controlled trial—SCORE. J Natl Cancer Inst. 2011;103:1310–1322. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
