

Standardized Treatment of Pulmonary Exacerbations (STOP) study: Physician treatment practices and outcomes for individuals with cystic fibrosis with pulmonary Exacerbations
- PMID: 28457954
- PMCID: PMC6581038
- DOI: 10.1016/j.jcf.2017.04.003
Standardized Treatment of Pulmonary Exacerbations (STOP) study: Physician treatment practices and outcomes for individuals with cystic fibrosis with pulmonary Exacerbations
Abstract
Background: Pulmonary Exacerbations (PEx) are associated with increased morbidity and mortality in individuals with CF. PEx management practices vary widely, and optimization through interventional trials could potentially improve outcomes. The object of this analysis was to evaluate current physician treatment practices and patient outcomes for PEx.
Methods: The Standardized Treatment of Pulmonary Exacerbations (STOP) observational study enrolled 220 participants ≥12years old admitted to the hospital for PEx at 11 U.S. CF centers. Spirometry and daily symptom scores were collected during the study. Physicians were surveyed on treatment goals and their management practices were observed. Treatment outcomes were compared to stated goals.
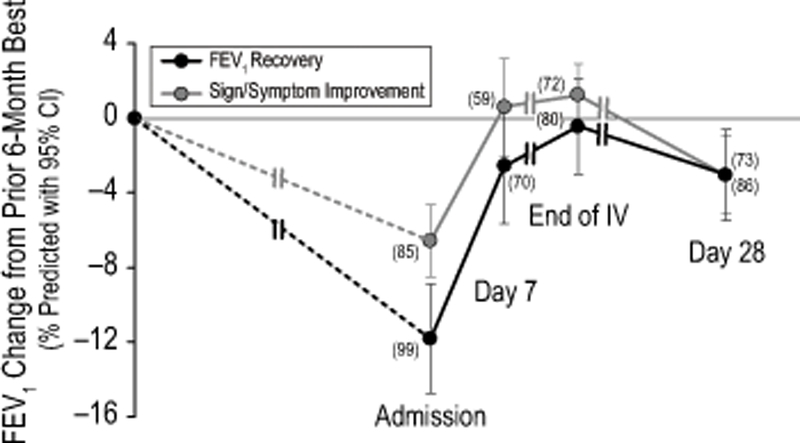
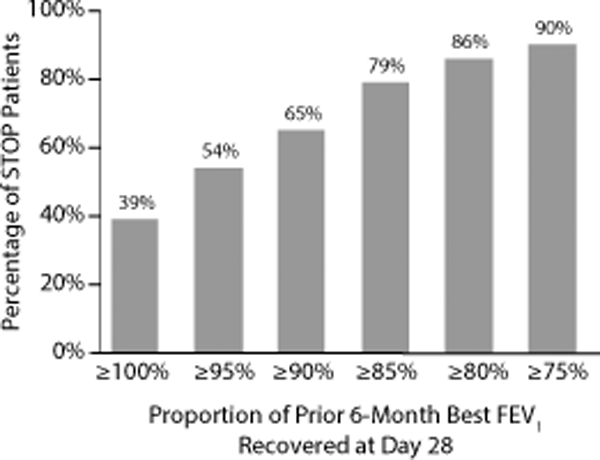
Results: The mean (SD) duration of IV antibiotic treatment was 15.9 (6.0) days. Those individuals with more severe lung disease (<50% FEV1) were treated nearly two days longer than those with >50% FEV1. Physician-reported FEV1 improvement goals were 10% (95% CI: 5%, 14%) lower for patients with 6-month baseline FEV1 ≤50% predicted compared with those with 6-month baseline FEV1 >50% predicted. There were clinically and statistically significant improvements in symptoms from the start of IV antibiotic treatment to the end of IV antibiotic treatment and 28days after the start of treatment. The mean absolute increase in FEV1 from admission was 9% predicted at end of IV antibiotic treatment, and 7% predicted at day 28. Only 39% fully recovered lost lung function, and only 65% recovered at least 90% of lost lung function. Treatment was deemed successful by 84% of clinicians, although 6-month baseline FEV1 was only recovered in 39% of PEx.
Conclusions: In this prospective observational study of PEx, treatment regimens and durations showed substantial variation. A significant proportion of patients did not reach physician's treatment goals, yet treatment was deemed successful.
Keywords: Antibiotic therapy; Cystic fibrosis; Physician treatment practices; Pulmonary Exacerbations.
Copyright © 2017 European Cystic Fibrosis Society. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures


Comment in
-
A first step to STOP cystic fibrosis exacerbations.J Cyst Fibros. 2017 Sep;16(5):529-531. doi: 10.1016/j.jcf.2017.08.006. J Cyst Fibros. 2017. PMID: 28865768 No abstract available.
References
-
- Sanders DB, Hoffman LR, Emerson J, Gibson RL, Rosenfeld M, Redding GJ, et al. Return of FEV1 after pulmonary exacerbation in children with cystic fibrosis. Pediatr Pulmonol. 2010. February;45(2):127–34. - PubMed
-
- Mayer-Hamblett N, Rosenfeld M, Emerson J, Goss CH, Aitken ML. Developing cystic fibrosis lung transplant referral criteria using predictors of 2-year mortality. Am J Respir Crit Care Med. 2002. December 15;166(12 Pt 1):1550–5. - PubMed
-
- Emerson J, Rosenfeld M, McNamara S, Ramsey B, Gibson RL. Pseudomonas aeruginosa and other predictors of mortality and morbidity in young children with cystic fibrosis. Pediatr Pulmonol. 2002. August;34(2):91–100. - PubMed
-
- Ellaffi M, Vinsonneau C, Coste J, Hubert D, Burgel PR, Dhainaut JF, et al. One-year outcome after severe pulmonary exacerbation in adults with cystic fibrosis. Am J Respir Crit Care Med. 2005. January 15;171(2):158–64. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
