

Community-directed mass drug administration is undermined by status seeking in friendship networks and inadequate trust in health advice networks
- PMID: 28458073
- PMCID: PMC5446315
- DOI: 10.1016/j.socscimed.2017.04.009
Community-directed mass drug administration is undermined by status seeking in friendship networks and inadequate trust in health advice networks
Abstract
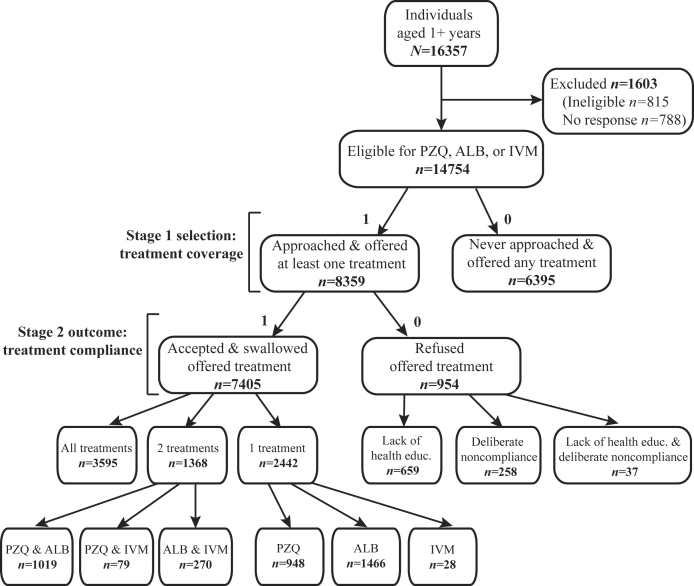
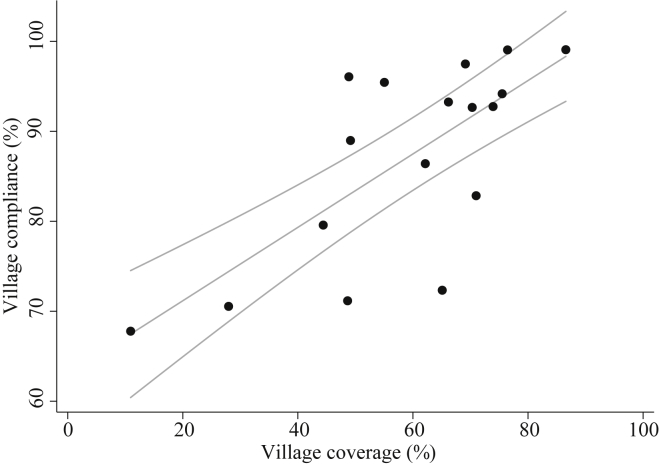
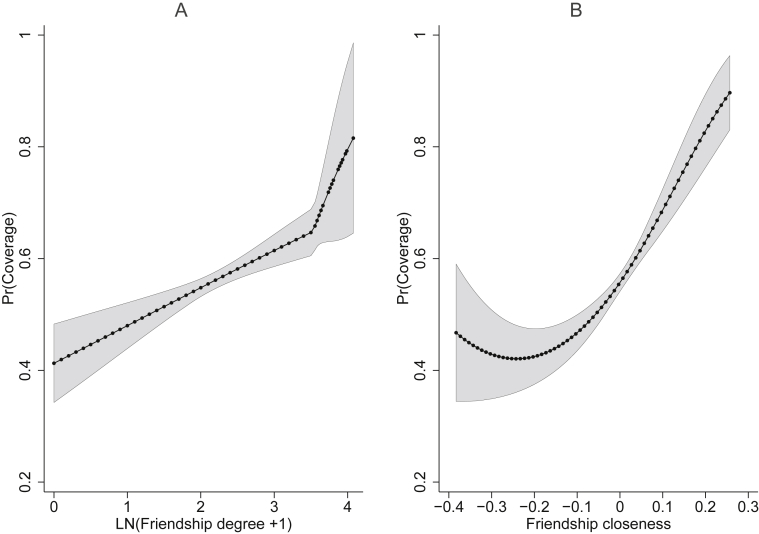
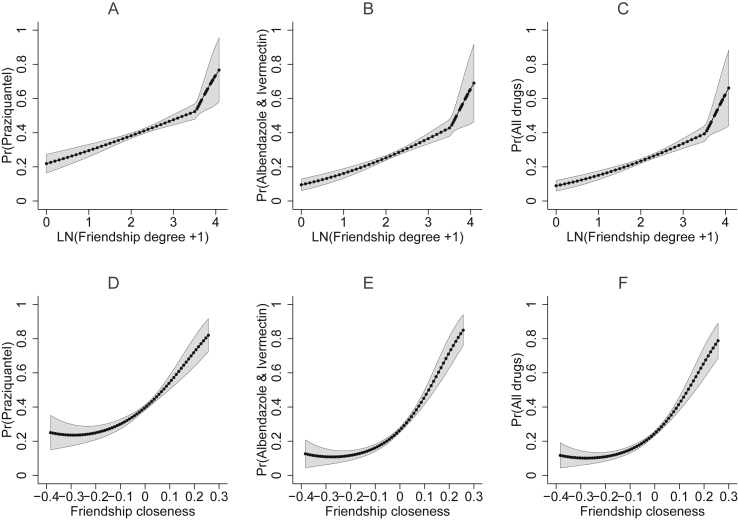
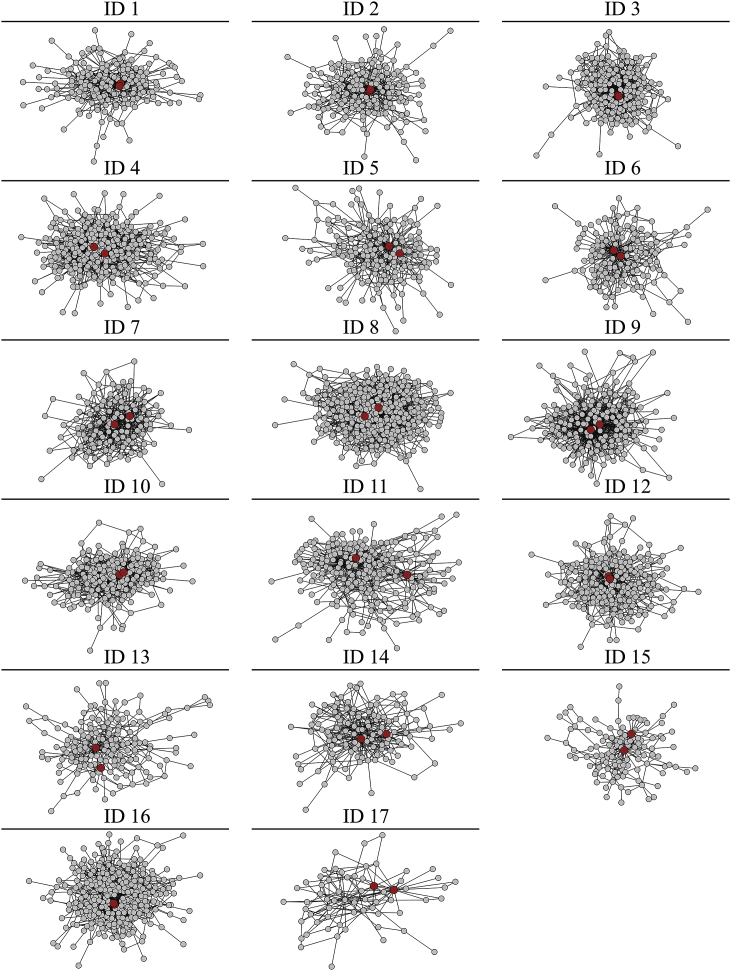
Over 1.9 billion individuals require preventive chemotherapy through mass drug administration (MDA). Community-directed MDA relies on volunteer community medicine distributors (CMDs) and their achievement of high coverage and compliance. Yet, it is unknown if village social networks influence effective MDA implementation by CMDs. In Mayuge District, Uganda, census-style surveys were conducted for 16,357 individuals from 3,491 households in 17 villages. Praziquantel, albendazole, and ivermectin were administered for one month in community-directed MDA to treat Schistosoma mansoni, hookworm, and lymphatic filariasis. Self-reported treatment outcomes, socioeconomic characteristics, friendship networks, and health advice networks were collected. We investigated systematically missed coverage and noncompliance. Coverage was defined as an eligible person being offered at least one drug by CMDs; compliance included ingesting at least one of the offered drugs. These outcomes were analyzed as a two-stage process using a Heckman selection model. To further assess if MDA through CMDs was working as intended, we examined the probability of accurate drug administration of 1) praziquantel, 2) both albendazole and ivermectin, and 3) all drugs. This analysis was conducted using bivariate Probit regression. Four indicators from each social network were examined: degree, betweenness centrality, closeness centrality, and the presence of a direct connection to CMDs. All models accounted for nested household and village standard errors. CMDs were more likely to offer medicines, and to accurately administer the drugs as trained by the national control programme, to individuals with high friendship degree (many connections) and high friendship closeness centrality (households that were only a short number of steps away from all other households in the network). Though high (88.59%), additional compliance was associated with directly trusting CMDs for health advice. Effective treatment provision requires addressing CMD biases towards influential, well-embedded individuals in friendship networks and utilizing health advice networks to increase village trust in CMDs.
Keywords: Compliance; Coverage; Mass drug administration; Social networks; Uganda.
Copyright © 2017 The Authors. Published by Elsevier Ltd.. All rights reserved.
Figures
References
-
- Albert R., Barabási A.-L. Statistical mechanics of complex networks. Rev. Mod. Phys. 2002;74(1):47–97.
-
- Ariely D., Bracha A., Meier S. Doing good or doing Well? Image motivation and monetary incentives in behaving prosocially. Am. Econ. Rev. 2009;99(1):544–555.
-
- Banerjee A., Chandrasekhar A.G., Duflo E., Jackson M.O. 2014. Gossip: Identifying Central Individuals in a Social Network.http://www.nber.org/papers/w20422 NBER Working Papers. No. 20422. Retrieved from:
-
- Bénabou R., Tirole J. Incentives and prosocial behavior. Am. Econ. Rev. 2006;96(5):1652–1678.
-
- Bester C.A., Conley T.G., Hansen C.B. Inference with dependent data using cluster covariance estimators. J. Econ. 2011;165(2):137–151.
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
