

Investigating the role of pentraxin 3 as a biomarker for bacterial infection in subjects with COPD
- PMID: 28458531
- PMCID: PMC5402921
- DOI: 10.2147/COPD.S123528
Investigating the role of pentraxin 3 as a biomarker for bacterial infection in subjects with COPD
Abstract
Background: Pentraxin 3 (PTX3) is an acute phase protein, involved in antibacterial resistance. Recent studies have shown PTX3 levels to be elevated in the presence of a bacterial infection and in a murine sepsis model.
Objective: We aim to investigate if sputum PTX3 can be used as a biomarker for bacterial infection in subjects with COPD.
Materials and methods: Sputum samples from 142 COPD patients (102 men) with a mean (range) age of 69 years (45-85) and mean (SD) post-bronchodilator percentage predicted forced expiratory volume in 1 second (FEV1) of 50% (19) were analyzed for PTX3, using a commercial assay at stable state and during an exacerbation. Association with bacteria, from culture, quantitative real-time polymerase chain reaction (qPCR) and colony-forming units (CFU) was investigated.
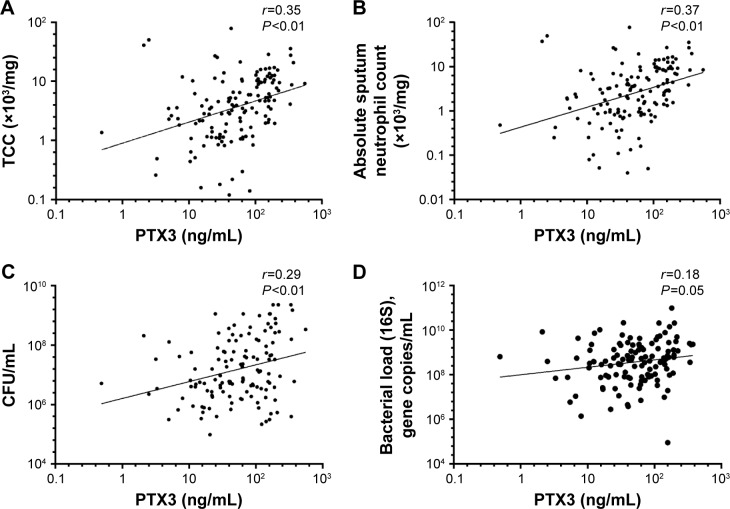
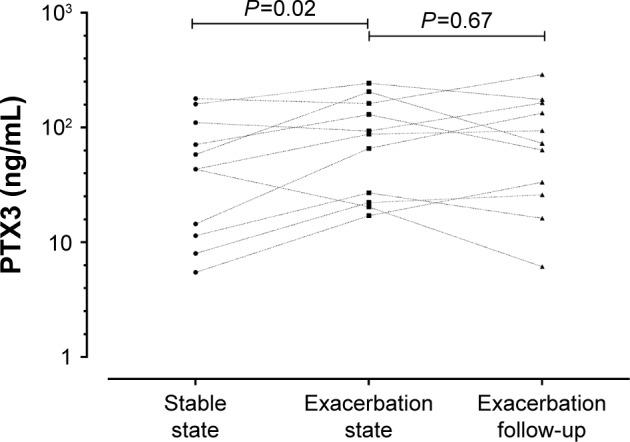
Results: The geometric mean (95% CI) PTX3 level at stable state was 50.5 ng/mL (41.4-61.7). PTX3 levels correlated with absolute neutrophil count in sputum (r=0.37; P<0.01), but not FEV1 or health status. There was a weak correlation between PTX3 and bacterial load (CFU: r=0.29, P<0.01; 16S qPCR: r=0.18, P=0.05). PTX3 was a poor predictor of bacterial colonization (defined as >105 CFU/mL at stable state) with a receiver-operating characteristic (ROC) area under the curve (AUC) of 0.59 and 95% confidence interval (CI) 0.43-0.76 (P=0.21). During an exacerbation, there was a modest increase in PTX3 (fold difference 0.15, 95% of difference 0.02-0.29; P=0.02), and PTX3 fared better at identifying a bacteria-associated exacerbation (ROC AUC 0.65, 95% CI 0.52-0.78, P=0.03).
Conclusion: PTX3 is associated with bacterial infection in patients with COPD, but its utility as a biomarker for identifying a bacteria-associated exacerbation warrants further studies.
Keywords: TNF-inducible gene 14 protein; infection; sputum.
Conflict of interest statement
Disclosure All authors declare no financial support from, or relationship with any organization that may have an interest, for the submitted work. MB is funded by a National Institute of Health Research (NIHR) Post-doctoral Fellowship (PDF-2013-06-052) and Oxford Health Sciences Research Committee. MB has received travel support from AstraZeneca, Boehringer Ingelheim, and GlaxoSmithKline and consultancy honoraria outside the submitted work from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, and Pfizer. CEB was funded by a Wellcome Trust Senior Fellowship. CEB has received grant support and consultancy honoraria outside the submitted work from AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Medimmune, Novartis, and Roche. The authors report no other conflicts of interest in this work.
Figures
References
-
- Vestbo J, Hurd SS, Agustí AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2013;187(4):347–365. - PubMed
-
- Garvey C. Recent updates in chronic obstructive pulmonary disease. Postgrad Med. 2016;128(2):231–238. - PubMed
-
- Bafadhel M, McKenna S, Terry S, et al. Acute exacerbations of chronic obstructive pulmonary disease: identification of biologic clusters and their biomarkers. Am J Respir Crit Care Med. 2011;184(6):662–671. - PubMed
-
- Monsó E, Ruiz J, Rosell A, et al. Bacterial infection in chronic obstructive pulmonary disease. A study of stable and exacerbated outpatients using the protected specimen brush. Am J Respir Crit Care Med. 1995;152(4):1316–1320. - PubMed
-
- Banerjee D, Khair OA, Honeybourne D. Impact of sputum bacteria on airway inflammation and health status in clinical stable COPD. Eur Respir J. 2004;23(5):685–691. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
