

Characteristics Detected on Computed Tomography Angiography Predict Coronary Artery Plaque Progression in Non-Culprit Lesions
- PMID: 28458601
- PMCID: PMC5390618
- DOI: 10.3348/kjr.2017.18.3.487
Characteristics Detected on Computed Tomography Angiography Predict Coronary Artery Plaque Progression in Non-Culprit Lesions
Abstract
Objective: This study sought to determine whether variables detected on coronary computed tomography angiography (CCTA) would predict plaque progression in non-culprit lesions (NCL).
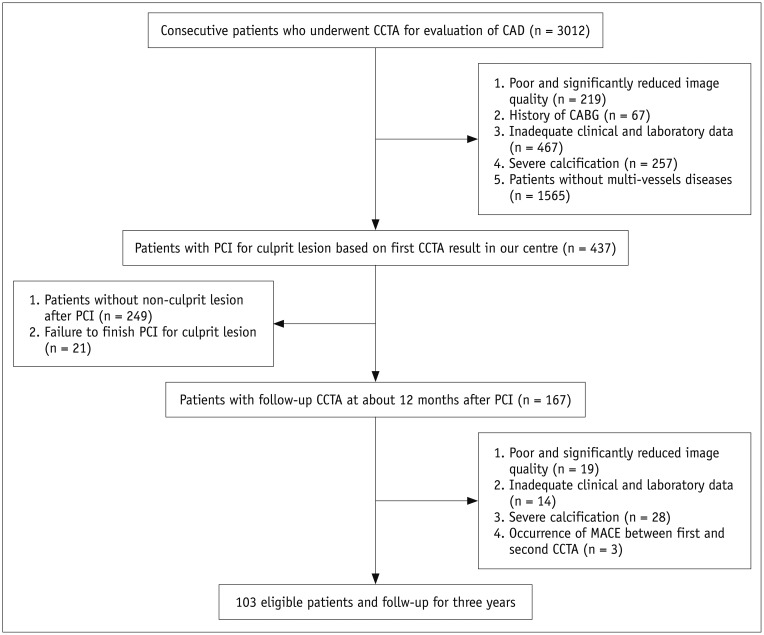
Materials and methods: In this single-center trial, we analyzed 103 consecutive patients who were undergoing CCTA and percutaneous coronary intervention (PCI) for culprit lesions. Follow-up CCTA was scheduled 12 months after the PCI, and all patients were followed for 3 years after their second CCTA examination. High-risk plaque features and epicardial adipose tissue (EAT) volume were assessed by CCTA. Each NCL stenosis grade was compared visually between two CCTA scans to detect plaque progression, and patients were stratified into two groups based on this. Logistic regression analysis was used to evaluate the factors that were independently associated with plaque progression in NCLs. Time-to-event curves were compared using the log-rank statistic.
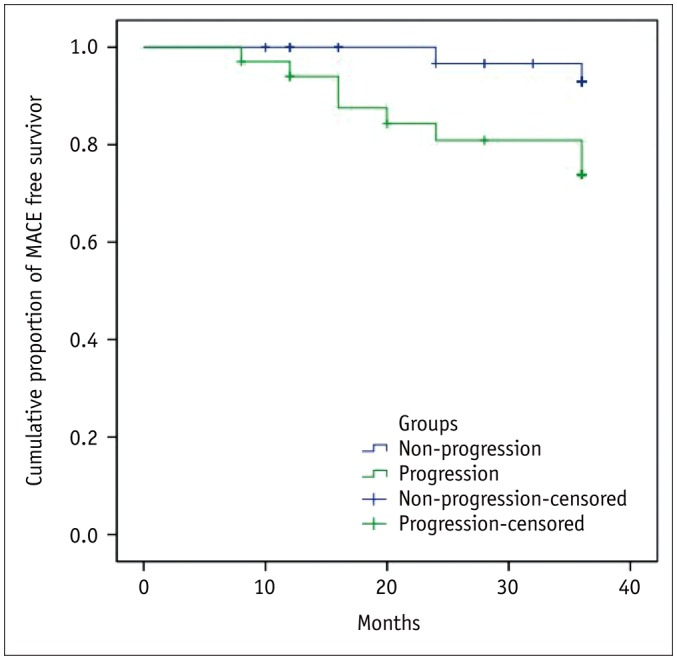
Results: Overall, 34 of 103 patients exhibited NCL plaque progression (33%). Logistic regression analyses showed that the NCL progression was associated with a history of ST-elevated myocardial infarction (odds ratio [OR] = 5.855, 95% confidence interval [CI] = 1.391-24.635, p = 0.016), follow-up low-density lipoprotein cholesterol level (OR = 6.832, 95% CI = 2.103-22.200, p = 0.001), baseline low-attenuation plaque (OR = 7.311, 95% CI = 1.242-43.028, p = 0.028) and EAT (OR = 1.015, 95% CI = 1.000-1.029, p = 0.044). Following the second CCTA examination, major adverse cardiac events (MACEs) were observed in 12 patients, and NCL plaque progression was significantly associated with future MACEs (log rank p = 0.006).
Conclusion: Noninvasive assessment of NCLs by CCTA has potential prognostic value.
Keywords: Coronary artery; Coronary computed tomography angiography; Epicardial adipose tissue; Low attenuation plaque; Non-culprit lesion; Plaque progression.
Figures
References
-
- Stone GW, Maehara A, Lansky AJ, de Bruyne B, Cristea E, Mintz GS, et al. A prospective natural-history study of coronary atherosclerosis. N Engl J Med. 2011;364:226–235. - PubMed
-
- Glaser R, Selzer F, Faxon DP, Laskey WK, Cohen HA, Slater J, et al. Clinical progression of incidental, asymptomatic lesions discovered during culprit vessel coronary intervention. Circulation. 2005;111:143–149. - PubMed
-
- Narula J, Kovacic JC. Putting TCFA in clinical perspective. J Am Coll Cardiol. 2014;64:681–683. - PubMed
-
- Motoyama S, Kondo T, Sarai M, Sugiura A, Harigaya H, Sato T, et al. Multislice computed tomographic characteristics of coronary lesions in acute coronary syndromes. J Am Coll Cardiol. 2007;50:319–326. - PubMed
-
- Motoyama S, Sarai M, Harigaya H, Anno H, Inoue K, Hara T, et al. Computed tomographic angiography characteristics of atherosclerotic plaques subsequently resulting in acute coronary syndrome. J Am Coll Cardiol. 2009;54:49–57. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
