

Novel Application of Quantitative Single-Photon Emission Computed Tomography/Computed Tomography to Predict Early Response to Methimazole in Graves' Disease
- PMID: 28458607
- PMCID: PMC5390624
- DOI: 10.3348/kjr.2017.18.3.543
Novel Application of Quantitative Single-Photon Emission Computed Tomography/Computed Tomography to Predict Early Response to Methimazole in Graves' Disease
Abstract
Objective: Since Graves' disease (GD) is resistant to antithyroid drugs (ATDs), an accurate quantitative thyroid function measurement is required for the prediction of early responses to ATD. Quantitative parameters derived from the novel technology, single-photon emission computed tomography/computed tomography (SPECT/CT), were investigated for the prediction of achievement of euthyroidism after methimazole (MMI) treatment in GD.
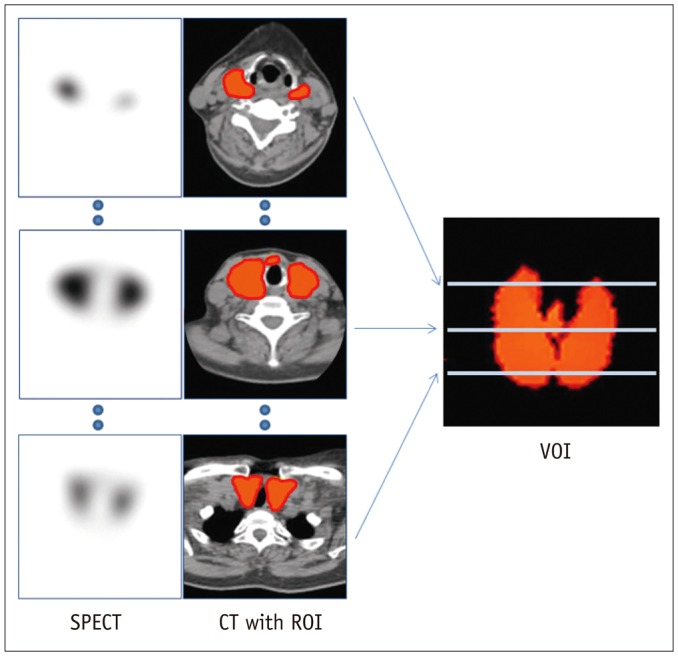
Materials and methods: A total of 36 GD patients (10 males, 26 females; mean age, 45.3 ± 13.8 years) were enrolled for this study, from April 2015 to January 2016. They underwent quantitative thyroid SPECT/CT 20 minutes post-injection of 99mTc-pertechnetate (5 mCi). Association between the time to biochemical euthyroidism after MMI treatment and %uptake, standardized uptake value (SUV), functional thyroid mass (SUVmean × thyroid volume) from the SPECT/CT, and clinical/biochemical variables, were investigated.
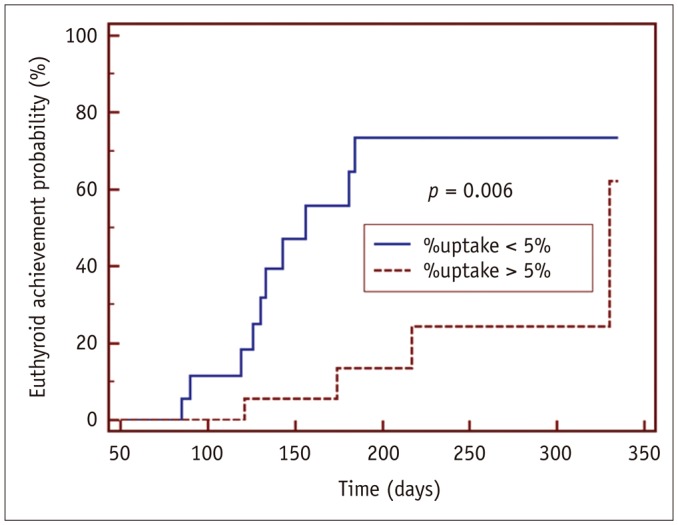
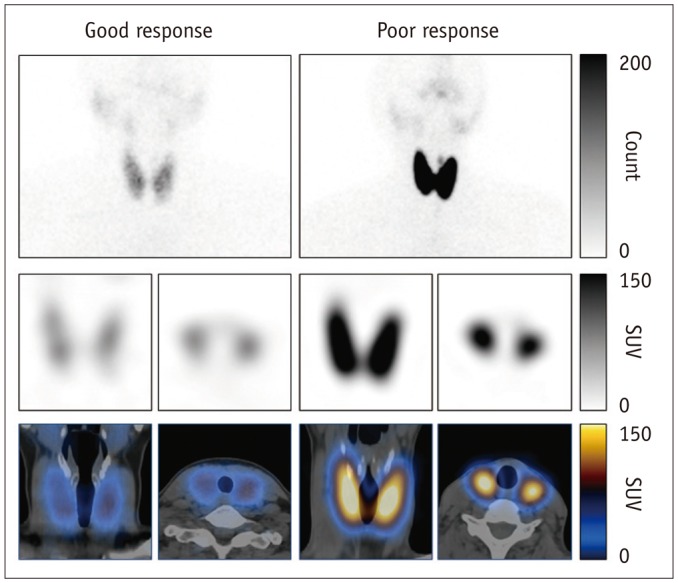
Results: GD patients had a significantly greater %uptake (6.9 ± 6.4%) than historical control euthyroid patients (n = 20, 0.8 ± 0.5%, p < 0.001) from the same quantitative SPECT/CT protocol. Euthyroidism was achieved in 14 patients at 156 ± 62 days post-MMI treatment, but 22 patients had still not achieved euthyroidism by the last follow-up time-point (208 ± 80 days). In the univariate Cox regression analysis, the initial MMI dose (p = 0.014), %uptake (p = 0.015), and functional thyroid mass (p = 0.016) were significant predictors of euthyroidism in response to MMI treatment. However, only %uptake remained significant in a multivariate Cox regression analysis (p = 0.034). A %uptake cutoff of 5.0% dichotomized the faster responding versus the slower responding GD patients (p = 0.006).
Conclusion: A novel parameter of thyroid %uptake from quantitative SPECT/CT is a predictive indicator of an early response to MMI in GD patients.
Keywords: Computed tomography; Euthyroidism; Graves' disease; Methimazole; Single-photon emission computed tomography.
Figures
Comment in
-
RE: Novel Application of Quantitative Single-Photon Emission Computed Tomography/Computed Tomography to Predict Early Response to Methimazole in Graves' Disease.Korean J Radiol. 2018 Jan-Feb;19(1):185-186. doi: 10.3348/kjr.2018.19.1.185. Epub 2018 Jan 2. Korean J Radiol. 2018. PMID: 29354016 Free PMC article. No abstract available.
References
-
- Brent GA. Clinical practice. Graves' disease. N Engl J Med. 2008;358:2594–2605. - PubMed
-
- Bahn Chair RS, Burch HB, Cooper DS, Garber JR, Greenlee MC, Klein I, et al. Hyperthyroidism and other causes of thyrotoxicosis: management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists. Thyroid. 2011;21:593–646. - PubMed
-
- Törring O, Tallstedt L, Wallin G, Lundell G, Ljunggren JG, Taube A, et al. Graves' hyperthyroidism: treatment with antithyroid drugs, surgery, or radioiodine--a prospective, randomized study. Thyroid Study Group. J Clin Endocrinol Metab. 1996;81:2986–2993. - PubMed
-
- Burch HB, Cooper DS. Management of Graves disease: a review. JAMA. 2015;314:2544–2554. - PubMed
-
- Vitti P, Rago T, Chiovato L, Pallini S, Santini F, Fiore E, et al. Clinical features of patients with Graves' disease undergoing remission after antithyroid drug treatment. Thyroid. 1997;7:369–375. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
