

Risks associated with viral infections during pregnancy
- PMID: 28459427
- PMCID: PMC5409792
- DOI: 10.1172/JCI87490
Risks associated with viral infections during pregnancy
Abstract
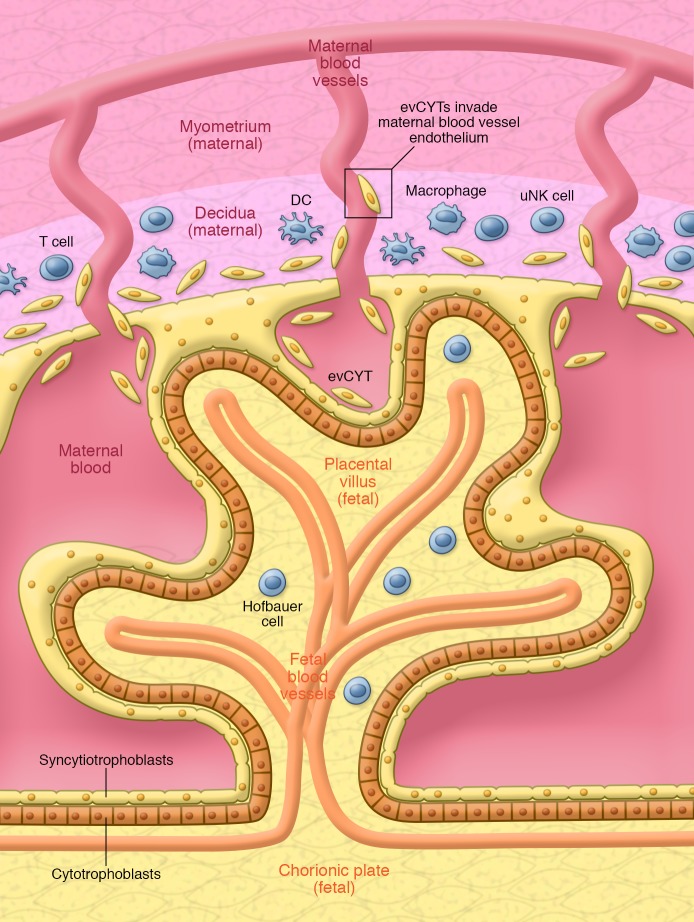
Despite the prevalence of viral infections in the American population, we still have a limited understanding of how they affect pregnancy and fetal development. Viruses can gain access to the decidua and placenta by ascending from the lower reproductive tract or via hematogenous transmission. Viral tropism for the decidua and placenta is then dependent on viral entry receptor expression in these tissues as well as on the maternal immune response to the virus. These factors vary by cell type and gestational age and can be affected by changes to the in utero environment and maternal immunity. Some viruses can directly infect the fetus at specific times during gestation, while some only infect the placenta. Both scenarios can result in severe birth defects or pregnancy loss. Systemic maternal viral infections can also affect the pregnancy, and these can be especially dangerous, because pregnant women suffer higher virus-associated morbidity and mortality than do nonpregnant counterparts. In this Review, we discuss the potential contributions of maternal, placental, and fetal viral infection to pregnancy outcome, fetal development, and maternal well-being.
Conflict of interest statement
Figures


References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
