

Biomechanical Analysis of Tibial Tuberosity Medialization and Medial Patellofemoral Ligament Reconstruction
- PMID: 28459747
- PMCID: PMC5412728
- DOI: 10.1097/JSA.0000000000000152
Biomechanical Analysis of Tibial Tuberosity Medialization and Medial Patellofemoral Ligament Reconstruction
Abstract
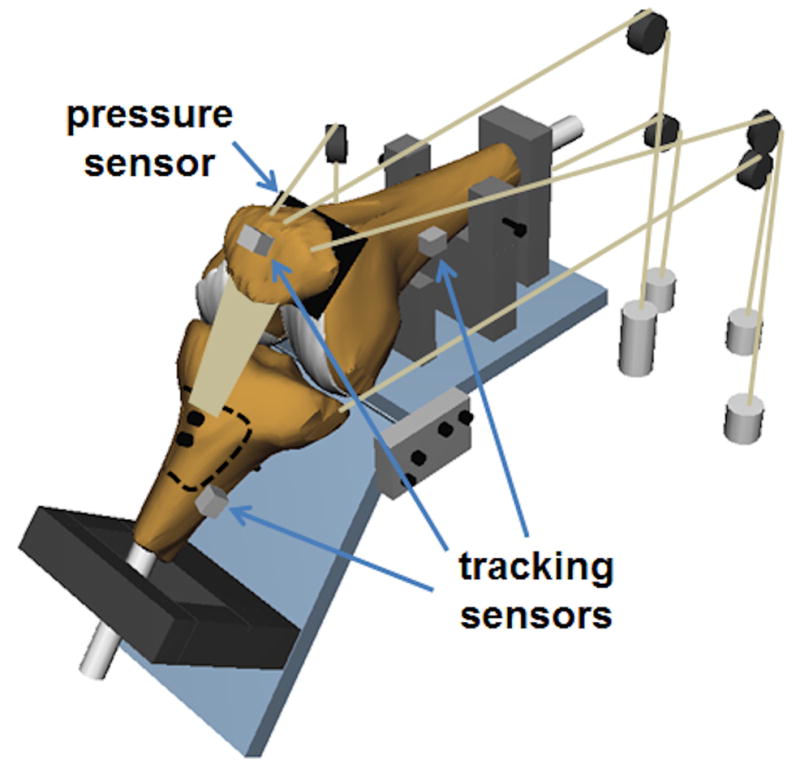
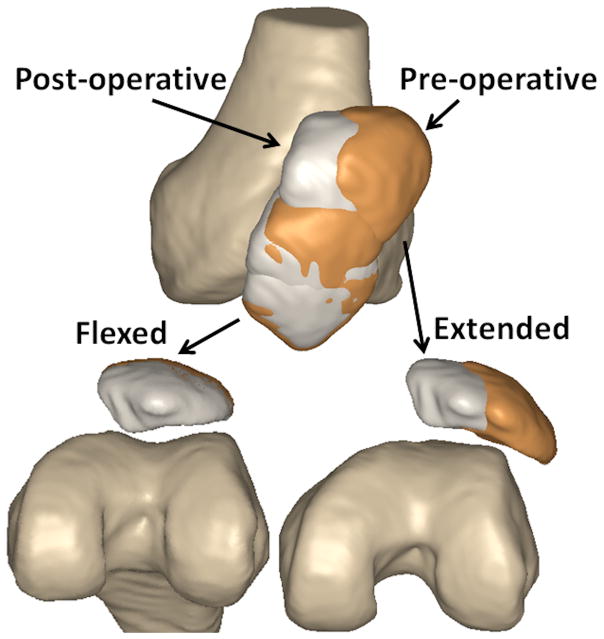
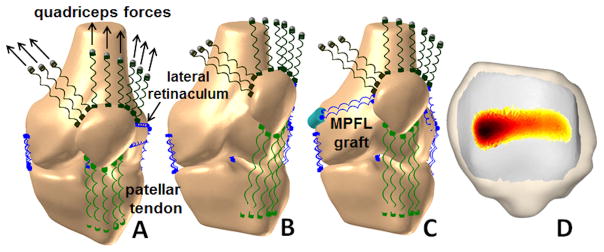
Biomechanical studies are commonly performed to evaluate the influence of medial patellofemoral ligament (MPFL) reconstruction and tibial tuberosity medialization on patellar tracking and patellofemoral contact pressures. The most common method is in vitro simulation of knee function, but computational simulation of knee function and computational reconstruction of in vivo motion can also be utilized. The current review of the biomechanical literature indicates that MPFL reconstruction and tibial tuberosity medialization reduce lateral patellar tracking. Decreased lateral patellofemoral contact pressures have also been noted. For MPFL reconstruction, the most commonly noted biomechanical concerns are graft overtensioning and nonanatomic attachment on the femur leading to overconstraint of the patella and elevated medial contact pressures. For tuberosity medialization, the influence of altered tibiofemoral kinematics on postoperative function is unknown. Future biomechanical studies should emphasize inclusion of anatomic features and tracking patterns related to patellar instability, with comparison between the surgical approaches for continued development of treatment guidelines.
Conflict of interest statement
Conflicts of Interest: None are declared for the remaining authors.
Figures
References
-
- Weber AE, Nathani A, Dines JS, et al. An algorithmic approach to the management of recurrent lateral patellar dislocation. J Bone Joint Surg Am. 2016;98:417–27. - PubMed
-
- Pritsch T, Haim A, Arbel R, et al. Tailored tibial tubercle transfer for patellofemoral malalignment: analysis of clinical outcomes. Knee Surg Sports Traumatol Arthrosc. 2007;15:994–1002. - PubMed
-
- Sherman SL, Erickson BJ, Cvetanovich GL, et al. Tibial tuberosity osteotomy: indications, techniques, and outcomes. Am J Sports Med. 2014;42:2006–17. - PubMed
-
- Schöttle PB, Schmeling A, Rosenstiel N, et al. Radiographic landmarks for femoral tunnel placement in medial patellofemoral ligament reconstruction. Am J Sports Med. 2007;35:801–4. - PubMed
-
- Stephen JM, Lumpaopong P, Deehan DJ, et al. The medial patellofemoral ligament: location of femoral attachment and length change patterns resulting from anatomic and nonanatomic attachments. Am J Sports Med. 2012;40:1871–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
