

Is Diabetes Mellitus a Risk Factor for Poor Outcomes after Left Ventricular Assist Device Placement?
- PMID: 28461796
- PMCID: PMC5408624
- DOI: 10.14503/THIJ-15-5698
Is Diabetes Mellitus a Risk Factor for Poor Outcomes after Left Ventricular Assist Device Placement?
Abstract
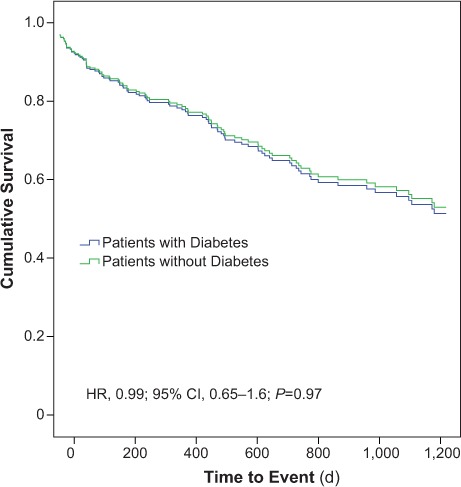
Diabetes mellitus is associated with adverse outcomes in patients with cardiovascular diseases, including heart failure. Left ventricular assist devices (LVADs) are increasingly used as life-saving therapy for advanced heart failure. The effects of pre-LVAD diabetes on long-term outcomes after LVAD implantation are not well understood. In this study, we retrospectively evaluated the effect of existing diabetes on post-LVAD outcomes. Data on 288 LVAD recipients from 2006 through 2013 were reviewed. Patients were stratified in accordance with their histories of diabetes. Baseline demographic, laboratory, hemodynamic, and echocardiographic information before LVAD placement were reviewed, together with the post-LVAD incidence of major adverse outcomes. Kaplan-Meier analysis and Cox regression analysis were performed. Our cohort comprised 122 patients with diabetes and 166 patients without. The mean glycosylated hemoglobin A1c level in the diabetes group was 7.4% ± 1.6%. Diabetic patients at baseline had a more adverse medical profile than did nondiabetic patients. There were no differences in major outcomes between the 2 groups other than a higher incidence of hemolysis in the diabetes group: 12 (10%) vs 5 (3%); P=0.02. There was no difference in survival outcomes between the groups. Diabetic patients did not have worse survival or more adverse outcomes than did nondiabetic patients in this study, perhaps because of improved diabetes control, or improvement in biochemical derangements after normalization of cardiac output with LVAD therapy. A diagnosis of diabetes was an independent predictor of hemolysis. Further studies to evaluate the link between hemolysis and diabetes are indicated.
Keywords: Diabetes mellitus/complications; heart failure; hemolysis; left ventricular assist devices; retrospective studies; treatment outcome.
Figures
Similar articles
-
Impact of Diabetes Mellitus on Outcomes in Patients Supported With Left Ventricular Assist Devices: A Single Institutional 9-Year Experience.Circ Heart Fail. 2017 Nov;10(11):e004213. doi: 10.1161/CIRCHEARTFAILURE.117.004213. Circ Heart Fail. 2017. PMID: 29141856
-
Clinical Impact of Diabetes Mellitus on Short-Term Outcomes andIn-Hospital Mortality of Cardiac Mechanical Support with Left Ventricular Assist Device (LVAD): A Retrospective Study from a National Database.Cardiovasc Revasc Med. 2019 Oct;20(10):883-886. doi: 10.1016/j.carrev.2018.12.011. Epub 2018 Dec 14. Cardiovasc Revasc Med. 2019. PMID: 30578171
-
Continuous-flow left ventricular assist device therapy in patients with preoperative hepatic failure: are we pushing the limits too far?Artif Organs. 2015 Apr;39(4):336-42. doi: 10.1111/aor.12375. Epub 2014 Oct 27. Artif Organs. 2015. PMID: 25345547
-
Predicting the Risk of Right Ventricular Failure in Patients Undergoing Left Ventricular Assist Device Implantation: A Systematic Review.Circ Heart Fail. 2020 Oct;13(10):e006994. doi: 10.1161/CIRCHEARTFAILURE.120.006994. Epub 2020 Sep 28. Circ Heart Fail. 2020. PMID: 32981331
-
Left Ventricular Assist Devices and the Kidney.Clin J Am Soc Nephrol. 2018 Feb 7;13(2):348-355. doi: 10.2215/CJN.04670417. Epub 2017 Oct 25. Clin J Am Soc Nephrol. 2018. PMID: 29070522 Free PMC article. Review.
Cited by
-
Left ventricular assist device implantation improves glycaemic control: a systematic review and meta-analysis.ESC Heart Fail. 2018 Dec;5(6):1141-1149. doi: 10.1002/ehf2.12337. Epub 2018 Jul 27. ESC Heart Fail. 2018. PMID: 30052326 Free PMC article.
-
Diabetes mellitus and risk of new-onset and recurrent heart failure: a systematic review and meta-analysis.ESC Heart Fail. 2020 Oct;7(5):2146-2174. doi: 10.1002/ehf2.12782. Epub 2020 Jul 29. ESC Heart Fail. 2020. PMID: 32725969 Free PMC article.
-
Impact of Diabetes and Glycemia on Cardiac Improvement and Adverse Events Following Mechanical Circulatory Support.J Am Heart Assoc. 2024 Jul 16;13(14):e032936. doi: 10.1161/JAHA.123.032936. Epub 2024 Jul 11. J Am Heart Assoc. 2024. PMID: 38989825 Free PMC article.
-
Influence of Diabetes Mellitus on Outcomes in Patients After Left Ventricular Assist Device Implantation.Ann Thorac Surg. 2018 Aug;106(2):555-560. doi: 10.1016/j.athoracsur.2018.02.045. Epub 2018 Mar 22. Ann Thorac Surg. 2018. PMID: 29577927 Free PMC article.
-
Impact of Diabetes Mellitus on Outcomes in Patients with Left Ventricular Assist Devices.Biomedicines. 2024 Jul 18;12(7):1604. doi: 10.3390/biomedicines12071604. Biomedicines. 2024. PMID: 39062177 Free PMC article. Review.
References
-
- Buse JB, Ginsberg HN, Bakris GL, Clark NG, Costa F, Eckel R, . et al. Primary prevention of cardiovascular diseases in people with diabetes mellitus: a scientific statement from the American Heart Association and the American Diabetes Association. Circulation 2007; 115( 1): 114– 26. - PubMed
-
- Kannel WB, Hjortland M, Castelli WP.. Role of diabetes in congestive heart failure: the Framingham study. Am J Cardiol 1974; 34( 1): 29– 34. - PubMed
-
- Nichols GA, Hillier TA, Erbey JR, Brown JB.. Congestive heart failure in type 2 diabetes: prevalence, incidence, and risk factors. Diabetes Care 2001; 24( 9): 1614– 9. - PubMed
-
- Owan TE, Redfield MM.. Epidemiology of diastolic heart failure. Prog Cardiovasc Dis 2005; 47( 5): 320– 32. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
