

Transcatheter Aortic Valve Implantation in a Patient with Unicuspid Aortic Valve
- PMID: 28461798
- PMCID: PMC5408626
- DOI: 10.14503/THIJ-15-5602
Transcatheter Aortic Valve Implantation in a Patient with Unicuspid Aortic Valve
Abstract
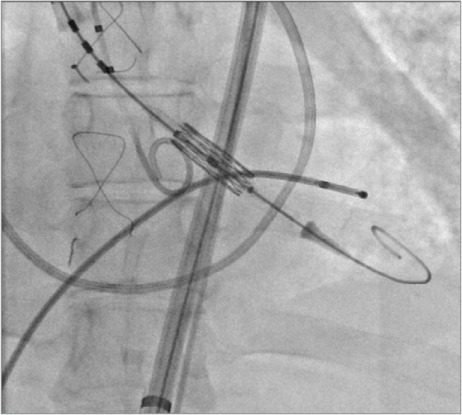
Transcatheter aortic valve replacement (TAVR) in patients with bicuspid aortic valves has been successfully performed, but there is a lack of published experience in percutaneous treatment of patients with unicuspid valves and severe aortic stenosis. We describe a case of TAVR in such a patient. A 31-year-old woman with Turner syndrome-who had undergone coarctation repair via subclavian flap at age 7 days and an aortic valvotomy at age 6 weeks-presented with severe symptomatic aortic stenosis. She was deemed inoperable because of her severe pulmonary hypertension and numerous comorbidities; consequently, a 20-mm Edwards Sapien 3 Transcatheter Heart Valve was offered for compassionate use. Postdeployment angiography and transesophageal echocardiography and aortography revealed no aortic insufficiency. Transcatheter aortic valve replacement for unicuspid aortic valve stenosis is technically feasible. Before implantation, particular attention should be paid to the interplay between the large single leaflet, coronary ostia, and stented valve, to select the correct size and position of the device. Some degree of intraoperative aortic migration should be anticipated.
Keywords: Aortic valve/abnormalities/pathology; aortic valve stenosis/therapy; cardiac catheterization/instrumentation; heart defects, congenital/complications; heart valve diseases; heart valve prosthesis implantation/methods.
Figures




References
-
- Edwards JE. Pathologic aspects of cardiac valvular insufficiencies. AMA Arch Surg 1958; 77( 4): 634– 49. - PubMed
-
- Roberts WC, Vowels TJ, Ko JM.. Natural history of adults with congenitally malformed aortic valves (unicuspid or bicuspid). Medicine (Baltimore) 2012; 91( 6): 287– 308. - PubMed
-
- Wijesinghe N, Ye J, Rodes-Cabau J, Cheung A, Velianou JL, Natarajan MK, . et al. Transcatheter aortic valve implantation in patients with bicuspid aortic valve stenosis. JACC Cardiovasc Interv 2010; 3( 11): 1122– 5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
