

Anterior cruciate ligament reconstruction: principles of treatment
- PMID: 28461919
- PMCID: PMC5367541
- DOI: 10.1302/2058-5241.1.160032
Anterior cruciate ligament reconstruction: principles of treatment
Abstract
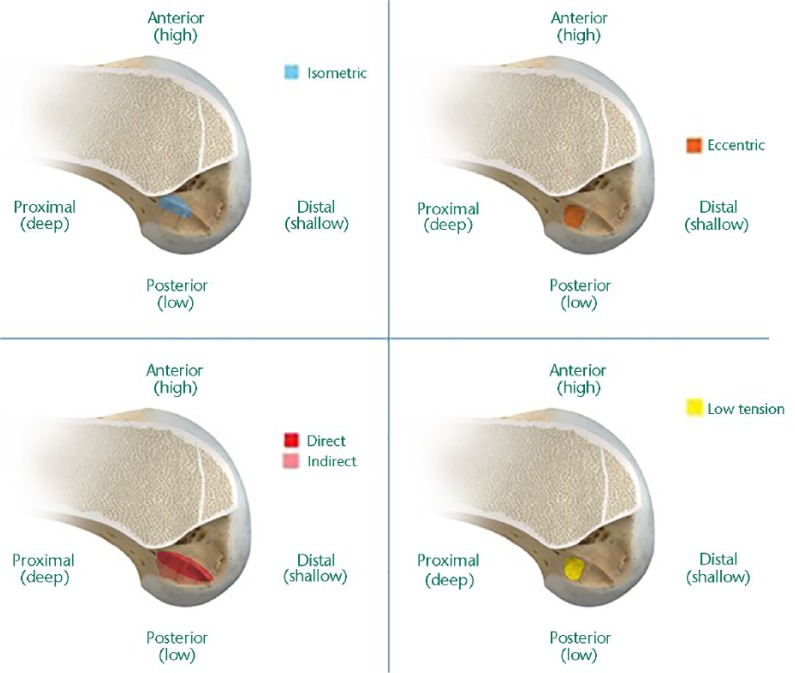
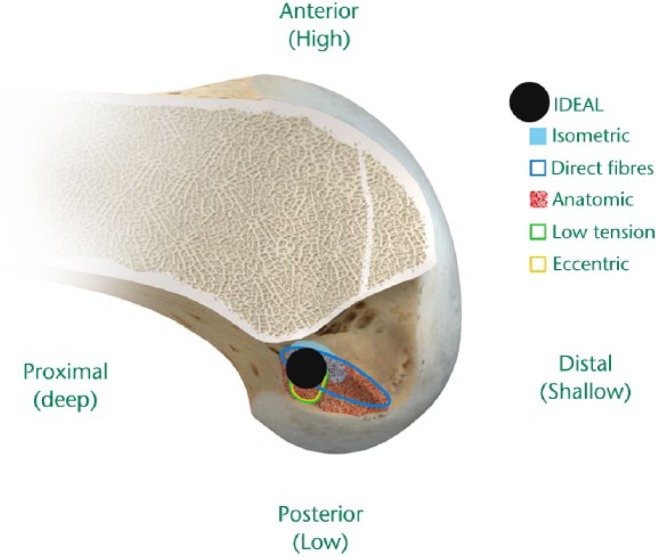
Anterior cruciate ligament (ACL) reconstruction is one of the most common procedures in sports medicine. Several areas of controversy exist in ACL tear management which have engaged surgeons and researchers in debates towards identifying an ideal approach for these patients.This instructional review discusses the principles of ACL reconstruction in an attempt to provide guidelines and initiate a critical thinking approach on the most common areas of controversy regarding ACL reconstruction.Using high-level evidence from the literature, as presented in randomised controlled trials, systematic reviews, and meta-analyses, operative versus conservative treatment, timing of surgery, and rehabilitation are discussed. Also, the advantages and disadvantages of the most common types of autografts, such as patellar tendon and hamstrings as well as allografts are presented.Key considerations for the anatomical, histological, biomechanical and clinical data ('IDEAL') graft positioning are reviewed. Cite this article: Paschos NK, Howell SM. Anterior cruciate ligament reconstruction: principles of treatment. EFORT Open Rev 2016;398-408. DOI: 10.1302/2058-5241.1.160032.
Keywords: ACL tear; allograft; anterior cruciate ligament; autograft; reconstruction; rehabilitation; timing; tunnel position.
Conflict of interest statement
Conflict of Interest: S. Howell reports personal fees from Zimmer Biomet, unconnected to this work.
Figures
References
-
- Griffin LY, Agel J, Albohm MJ, et al. Noncontact anterior cruciate ligament injuries: risk factors and prevention strategies. J Am Acad Orthop Surg 2000;8:141-150. - PubMed
-
- Mall NA, Chalmers PN, Moric M, et al. Incidence and trends of anterior cruciate ligament reconstruction in the United States. Am J Sports Med 2014;42:2363-2370. - PubMed
-
- Parkkari J, Pasanen K, Mattila VM, Kannus P, Rimpelä A. The risk for a cruciate ligament injury of the knee in adolescents and young adults: a population-based cohort study of 46 500 people with a 9 year follow-up. Br J Sports Med 2008;42:422-426. - PubMed
-
- Prodromos CC, Han Y, Rogowski J, Joyce B, Shi K. A meta-analysis of the incidence of anterior cruciate ligament tears as a function of gender, sport, and a knee injury-reduction regimen. Arthroscopy 2007;23:1320-5 e6. - PubMed
-
- Pearle AD, McAllister D, Howell SM. Rationale for strategic graft placement in anterior cruciate ligament reconstruction: I.D.E.A.L. femoral tunnel position. Am J Orthop (Belle Mead NJ) 2015;44:253-258. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
