

Complications in reverse shoulder arthroplasty
- PMID: 28461931
- PMCID: PMC5367530
- DOI: 10.1302/2058-5241.1.160003
Complications in reverse shoulder arthroplasty
Abstract
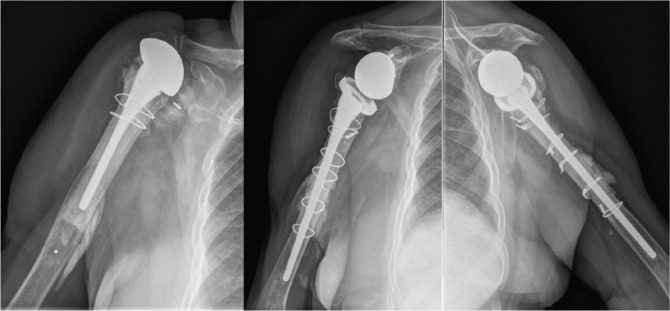
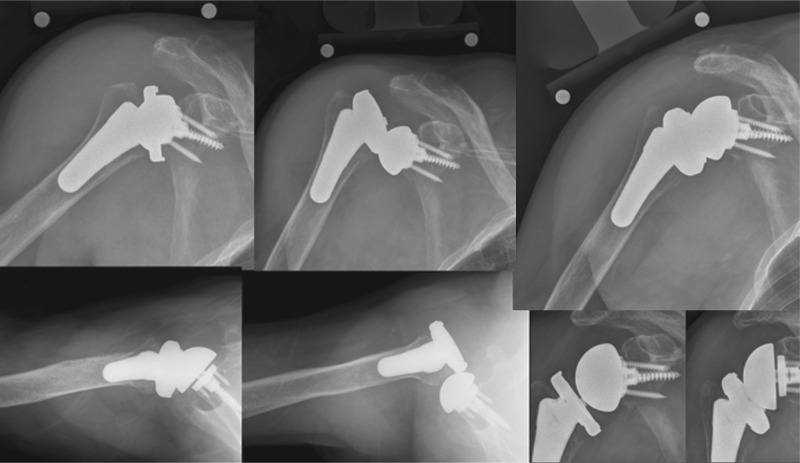
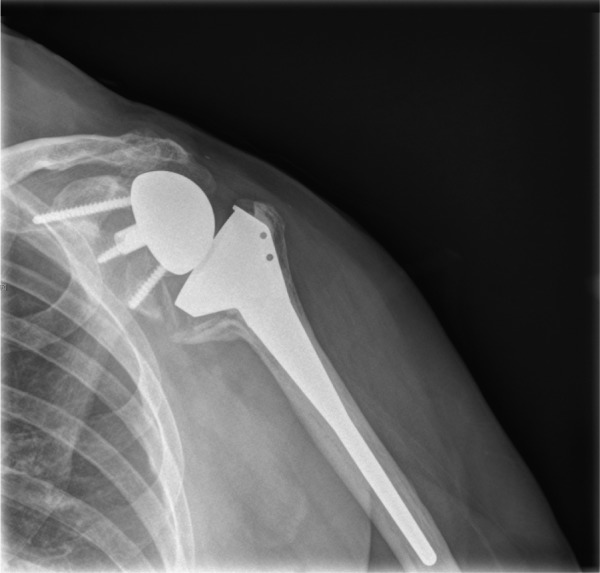
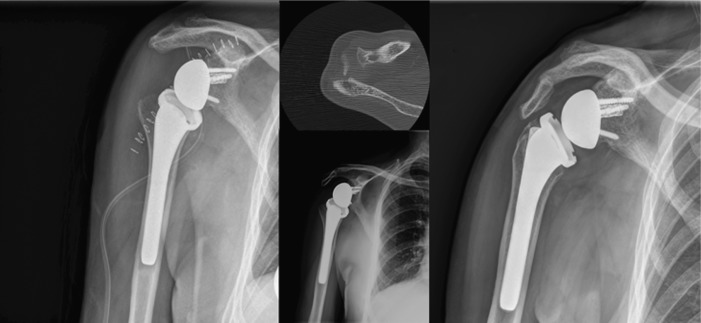
The reported rate of complications of reverse shoulder arthroplasty (RSA) seems to be higher than the complication rate of anatomical total shoulder arthroplasty.The reported overall complication rate of primary RSA is approximately 15%; when RSA is used in the revision setting, the complication rate may approach 40%.The most common complications of RSA include instability, infection, notching, loosening, nerve injury, acromial and scapular spine fractures, intra-operative fractures and component disengagement.Careful attention to implant design and surgical technique, including implantation of components in the correct version and height, selection of the best glenosphere-humeral bearing match, avoidance of impingement, and adequate management of the soft tissues will hopefully translate in a decreasing number of complications in the future. Cite this article: Barco R, Savvidou OD, Sperling JW, Sanchez-Sotelo J, Cofield RH. Complications in reverse shoulder arthroplasty. EFORT Open Rev 2016;1:72-80. DOI: 10.1302/2058-5241.1.160003.
Keywords: Complications; fracture; instability; loosening; notching; reverse shoulder arthroplasty.
Conflict of interest statement
Conflict of interest: J.W. Sperling has received royalties from Zimmer-Biomet; J. Sanchez-Sotelo has received royalties from Stryker and Zimmer-Biomet, and has carried out consultancy for Stryker; R.H. Cofield has received royalties from Smith and Nephew.
Figures

References
-
- Grammont PM, Baulot E. Delta shoulder prosthesis for rotator cuff rupture. Orthopedics 1993;16:65-68. PMID:8421661. - PubMed
-
- Ek ET, Neukom L, Catanzaro S, Gerber C. Reverse total shoulder arthroplasty for massive irreparable rotator cuff tears in patients younger than 65 years old: results after five to fifteen years. J Shoulder Elbow Surg 2013;22:1199-1208. PMID:23385083. - PubMed
-
- Holcomb JO, Hebert DJ, Mighell MA, et al. Reverse shoulder arthroplasty in patients with rheumatoid arthritis. J Shoulder Elbow Surg 2010;19:1076-1084. PMID:20363159. - PubMed
-
- Raiss P, Edwards TB, da Silva MR, Bruckner T, Loew M, Walch G. Reverse shoulder arthroplasty for the treatment of nonunions of the surgical neck of the proximal part of the humerus (type-3 fracture sequelae). J Bone Joint Surg [Am] 2014;96:2070-2076. PMID:25520341. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
