

Patella instability in children and adolescents
- PMID: 28461943
- PMCID: PMC5367529
- DOI: 10.1302/2058-5241.1.000018
Patella instability in children and adolescents
Abstract
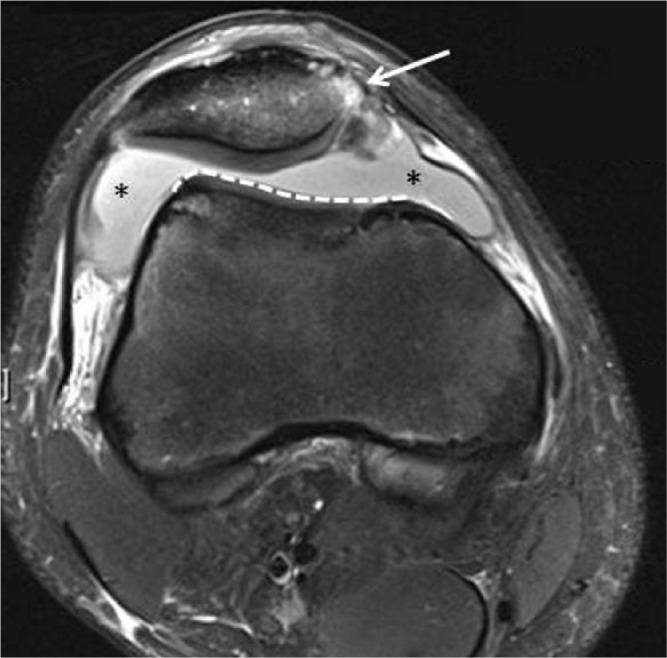
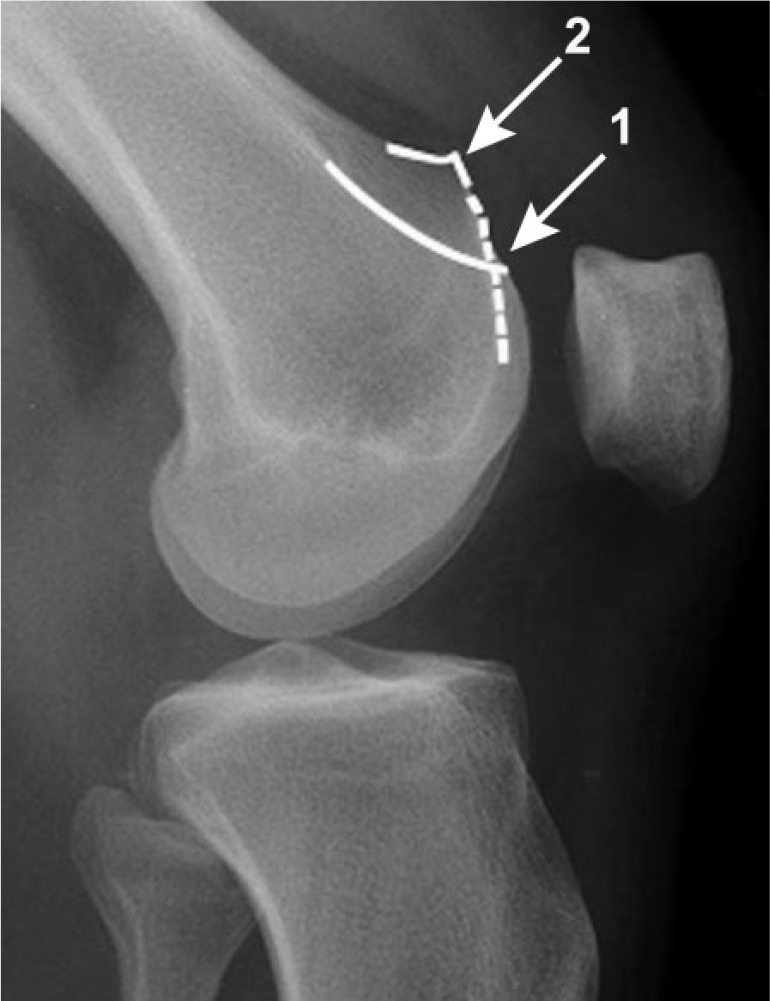
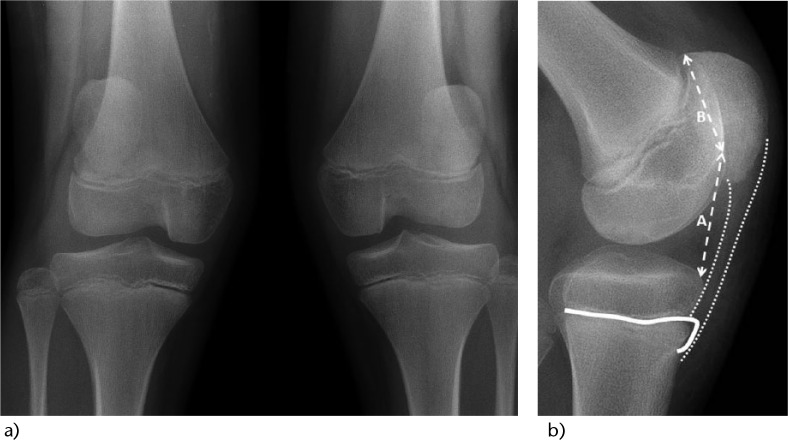
Patellar instabilities are the most common knee pathologies during growth. Congenital dislocations are rare. Extensive, early soft tissue releases relocate the extensor mechanism and may enable normal development of the femoro-patellar anatomy.Conservative management is the preferred strategy after a 'first-time' traumatic dislocation. In cases with concomitant anatomical predisposing factors such as trochlear dysplasia, malalignment, malrotation or ligamentous laxity, surgical reconstruction must be considered. The same applies to recurrent dislocations with pain, a sense of instability or re-dislocations which may also lead to functional compensatory mechanisms (quadriceps-avoiding gait in knee extension) or cartilaginous lesions with subsequent patello-femoral osteoarthritis. The decision-making process guiding surgical re-alignment includes analysis with standard radiographs and MRI of the trochlear groove, joint cartilage and medial patello-femoral ligament (MPFL). Careful evaluation of dynamic and static stabilisers is essential: the medial patello-femoral ligament provides stability during the first 20° of flexion, and the trochlear groove thereafter.Excessive femoral anteversion, general ligamentous laxity with increased femoro-tibial rotation, patella alta and increased distance between the tibial tuberosity and the trochlear groove must also be taken into account and surgically corrected.In cases with ongoing dislocations during skeletal immaturity, soft tissue procedures must suffice: reconstruction of the medial patello-femoral ligament as a standalone procedure or in conjuction with more complex distal realignment of the quadriceps mechanism may lead to a permanent stable result, or at least buys time until a definitive bony procedure is performed. Cite this article: Hasler CC, Studer D. Patella instability in children and adolescents. EFORT Open Rev 2016;1:160-166. DOI: 10.1302/2058-5241.1.000018.
Keywords: dysplasia; medial patellofemoral ligament; patellar dislocation (habitual; recurrent); trochlea.
Conflict of interest statement
Conflict of Interest: CH has received financial support outside of the current work in the form of consultancy fees from DePuy Synthes.
Figures
References
-
- Nietosvaara Y, Aalto K, Kallio PE. Acute patellar dislocation in children: incidence and associated osteochondral fractures. J Pediatr Orthop 1994;14:513-5. PMID: 8077438. - PubMed
-
- Fithian DC, Paxton EW, Stone ML, et al. Epidemiology and natural history of acute patellar dislocation. Am J Sports Med 2004;32:1114-21. PMID: 15262631. - PubMed
-
- Lewallen LW, McIntosh AL, Dahm DL. Predictors of recurrent instability after acute patellofemoral dislocation in pediatric and adolescent patients. Am J Sports Med 2013;41:575-81. PMID: 23339838. - PubMed
-
- Sanfridsson J, Arnbjornsson A, Friden T, Ryd L, Svahn G, Jonsson K. Femorotibial rotation and the Q-angle related to the dislocating patella. Acta Radiol 2001;42:218-24. PMID: 11259951. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
