

Treatment strategy for tibial plateau fractures: an update
- PMID: 28461952
- PMCID: PMC5367528
- DOI: 10.1302/2058-5241.1.000031
Treatment strategy for tibial plateau fractures: an update
Abstract
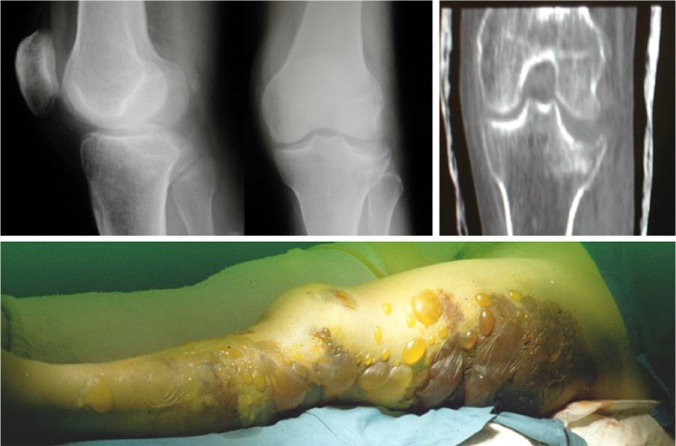
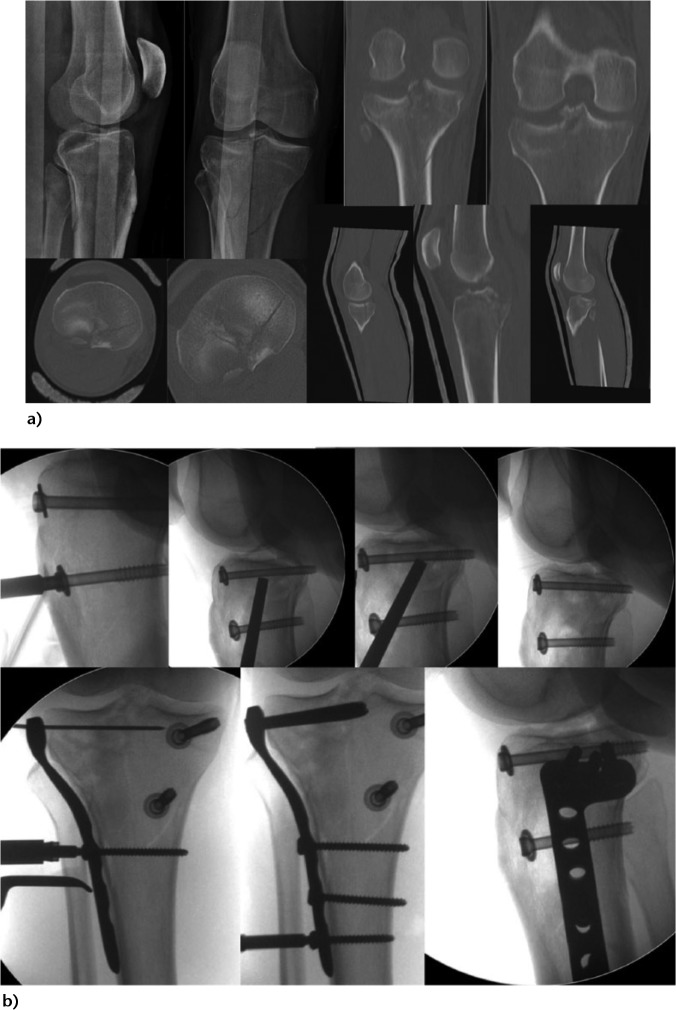
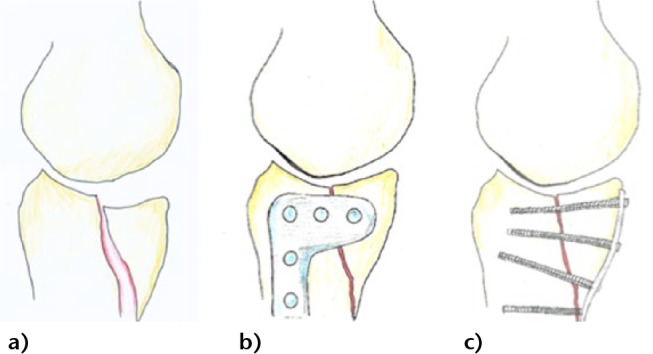
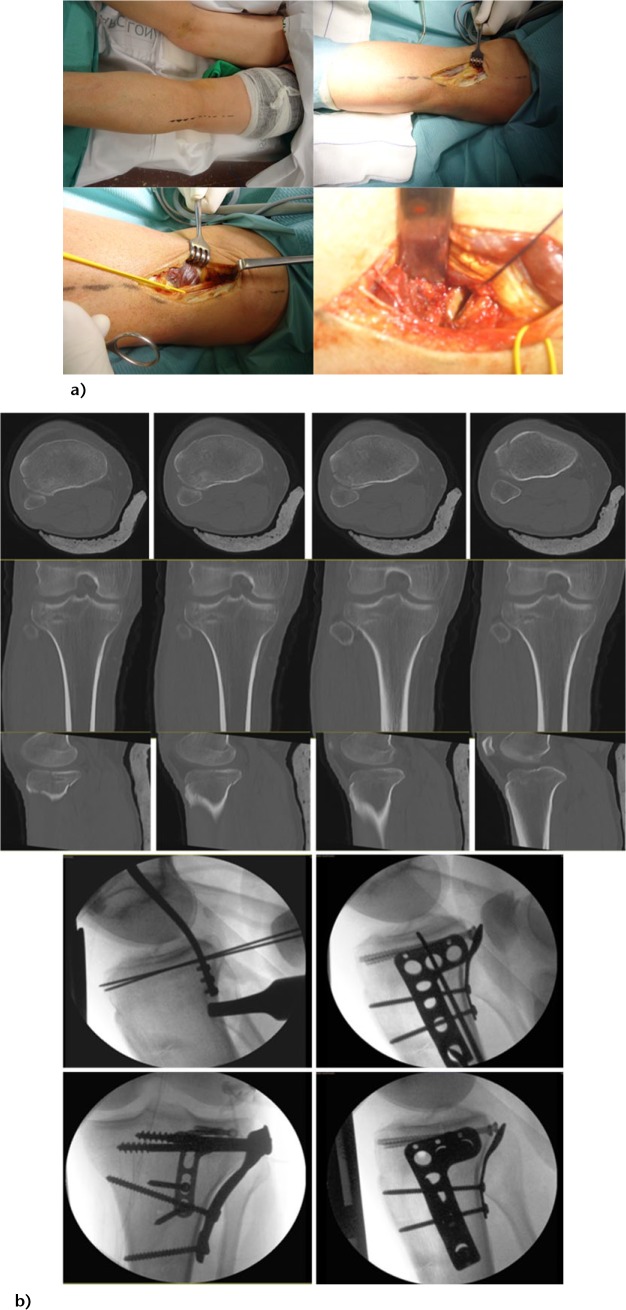
Tibial plateau fractures are complex injuries produced by high- or low-energy trauma. They principally affect young adults or the 'third age' population.These fractures usually have associated soft-tissue lesions that will affect their treatment. Sequential (staged) treatment (external fixation followed by definitive osteosynthesis) is recommended in more complex fracture patterns. But one should remember that any type of tibial plateau fracture can present with soft-tissue complications.Typically the Schatzker or AO/OTA classification is used, but the concept of the proximal tibia as a three-column structure and the detailed study of the posteromedial and posterolateral fragment morphology has changed its treatment strategy.Limb alignment and articular surface restoration, allowing early knee motion, are the main goals of surgical treatment. Partially articular factures can be treated by minimally-invasive methods and arthroscopy is useful to assist and control the fracture reduction and to treat intra-articular soft-tissue injuries.Open reduction and internal fixation (ORIF) is the gold standard treatment for these fractures. Complex articular fractures can be treated by ring external fixators and minimally-invasive osteosynthesis (EFMO) or by ORIF. EFMO can be related to suboptimal articular reduction; however, outcome analysis shows results that are equal to, or even superior to, ORIF. The ORIF strategy should also include the optimal reduction of the articular surface.Anterolateral and anteromedial surgical approaches do not permit adequate reduction and fixation of posterolateral and posteromedial fragments. To achieve this, it is necessary to reduce and fix them through specific posterolateral or posteromedial approaches that allow optimal reduction and plate/screw placement.Some authors have also suggested that primary total knee arthroplasty could be an option in specific patients and with specific fracture patterns. Cite this article: Prat-Fabregat S, Camacho-Carrasco P. Treatment strategy for tibial plateau fractures: an update. EFORT Open Rev 2016;1:225-232. DOI: 10.1302/2058-5241.1.000031.
Keywords: posterolateral knee approach; posteromedial knee approach; staged sequential surgical treatment; three-column concept; tibial plateau fractures.
Conflict of interest statement
Conflict of Interest: None declared.
Figures
References
-
- Borrelli J., Jr Management of soft tissue injuries associated with tibial plateau fractures. J Knee Surg 2014;27:5-9. - PubMed
-
- Hall JA, Beuerlein MJ, McKee M, Canadian Orthopaedic Trauma Society. Open Reduction and Internal Fixation Compared with Circular Fixator Application for Bicondylar Tibial Plateau Fractures. J Bone Jt Surg 2009;91:74-8. - PubMed
-
- Lowe JA, Tejwani N, Yoo B, Wolinsky P. Surgical techniques for complex proximal tibial fractures. J Bone Joint Surg [Am] 2011;93-A:1548-59. - PubMed
-
- Südkamp NP. Soft-tissue injury: pathophysiology and its influence on fracture management. In: Reudi TP, Murphy WM, eds. AO Principles of Fracture Management Stuttgart, Germany: Thieme, 2000:59-77.
-
- Giordano CP, Koval KJ, Zuckerman JD, Desai P. Fracture blisters. Clin Orthop Relat Res 1994;307:214-21. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
