

Identifying sources, pathways and risk drivers in ecosystems of Japanese Encephalitis in an epidemic-prone north Indian district
- PMID: 28463989
- PMCID: PMC5412994
- DOI: 10.1371/journal.pone.0175745
Identifying sources, pathways and risk drivers in ecosystems of Japanese Encephalitis in an epidemic-prone north Indian district
Abstract
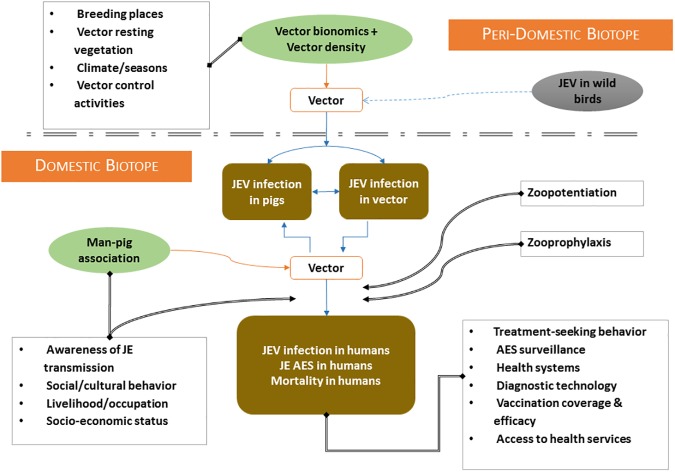
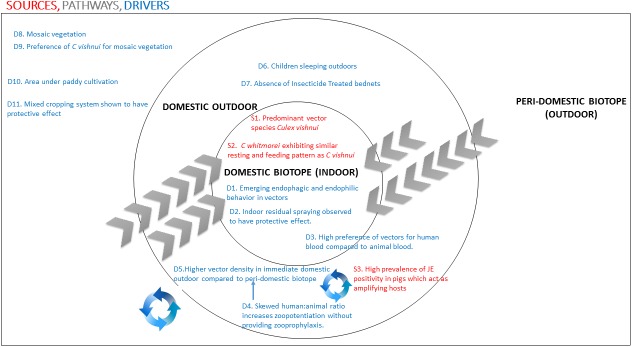
Japanese Encephalitis (JE) has caused repeated outbreaks in endemic pockets of India. This study was conducted in Kushinagar, a highly endemic district, to understand the human-animal-ecosystem interactions, and the drivers that influence disease transmission. Utilizing the ecosystems approach, a cross-sectional, descriptive study, employing mixed methods design was employed. Four villages (two with pig-rearing and two without) were randomly selected from a high, a medium and a low burden (based on case counts) block of Kushinagar. Children, pigs and vectors were sampled from these villages. A qualitative arm was incorporated to explain the findings from the quantitative surveys. All human serum samples were screened for JE-specific IgM using MAC ELISA and negative samples for JE RNA by rRT-PCR in peripheral blood mononuclear cells. In pigs, IgG ELISA and rRT-PCR for viral RNA were used. Of the 242 children tested, 24 tested positive by either rRT-PCR or MAC ELISA; in pigs, 38 out of the 51 pigs were positive. Of the known vectors, Culex vishnui was most commonly isolated across all biotopes. Analysis of 15 blood meals revealed human blood in 10 samples. Univariable analysis showed that gender, religion, lack of indoor residual spraying of insecticides in the past year, indoor vector density (all species), and not being vaccinated against JE in children were significantly associated with JE positivity. In multivariate analysis, only male gender remained as a significant risk factor. Based on previous estimates of symptomatic: asymptomatic cases of JE, we estimate that there should have been 618 cases from Kushinagar, although only 139 were reported. Vaccination of children and vector control measures emerged as major control activities; they had very poor coverage in the studied villages. In addition, lack of awareness about the cause of JE, lack of faith in the conventional medical healthcare system and multiple referral levels causing delay in diagnosis and treatment emerged as factors likely to result in adverse clinical outcomes.
Conflict of interest statement
Figures
References
-
- Ghosh D, Basu A. Japanese encephalitis-a pathological and clinical perspective. PLoS Negl Trop Dis. Public Library of Science; 2009;3: e437 doi: 10.1371/journal.pntd.0000437 - DOI - PMC - PubMed
-
- Pieper SJ, Kurland LT. Sequelae of Japanese B and mumps encephalitis: recent follow-up of patients affected in 1947–1948 epidemic on Guam. Am J Trop Med Hyg. 1958;7: 481–90. Available: http://www.ncbi.nlm.nih.gov/pubmed/13571562 - PubMed
-
- Kakoti G, Dutta P, Ram Das B, Borah J, Mahanta J. Clinical profile and outcome of Japanese encephalitis in children admitted with acute encephalitis syndrome. Biomed Res Int. Hindawi Publishing Corporation; 2013;2013: 152656 doi: 10.1155/2013/152656 - DOI - PMC - PubMed
-
- Baruah HC, Biswas D, Patgiri D, Mahanta J. Clinical outcome and neurological sequelae in serologically confirmed cases of Japanese encephalitis patients in Assam, India. Indian Pediatr. 2002;39: 1143–8. Available: http://www.ncbi.nlm.nih.gov/pubmed/12522277 - PubMed
-
- Carey DE, Myers RM, Pavri KM. Japanese encephalitis studies in Vellore, South India. II. Antibody response of patients. Indian J Med Res. 1968;56: 1319–29. Available: http://www.ncbi.nlm.nih.gov/pubmed/4302907 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
