

Increasing colonoscopy screening in disparate populations: Results from an evaluation of patient navigation in the New Hampshire Colorectal Cancer Screening Program
- PMID: 28464213
- PMCID: PMC5892823
- DOI: 10.1002/cncr.30761
Increasing colonoscopy screening in disparate populations: Results from an evaluation of patient navigation in the New Hampshire Colorectal Cancer Screening Program
Abstract
Background: To investigate uniformly successful results from a statewide program of patient navigation (PN) for colonoscopy, this comparison study evaluated the effectiveness of the PN intervention by comparing outcomes for navigated versus non-navigated patients in one of the community health clinics included in the statewide program. Outcomes measured included screening completion, adequacy of bowel preparation, missed appointments and cancellations, communication of test results, and consistency of follow-up recommendations with clinical guidelines.
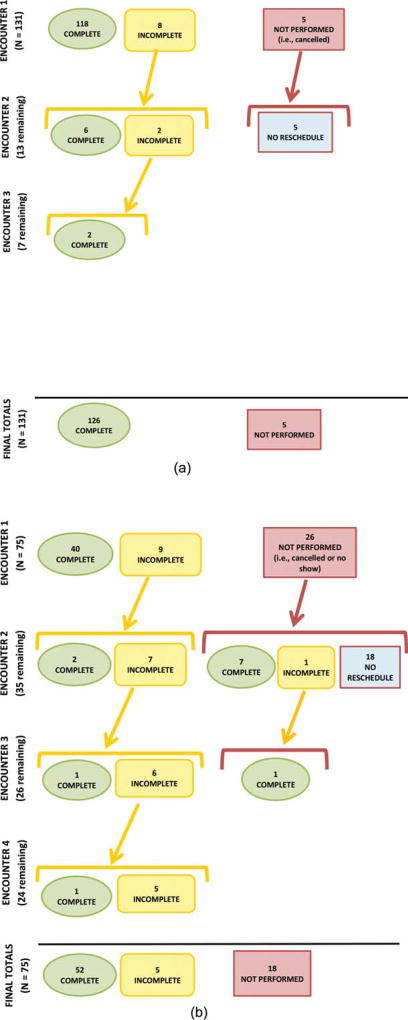
Methods: The authors compared a subset of 131 patients who were navigated to a screening or surveillance colonoscopy with a similar subset of 75 non-navigated patients at one endoscopy clinic. The prevalence and prevalence odds ratios were computed to measure the association between PN and each study outcome measure.
Results: Patients in the PN intervention group were 11.2 times more likely to complete colonoscopy than control patients (96.2% vs 69.3%; P<.001), and were 5.9 times more likely to have adequate bowel preparation (P =.010). In addition, intervention patients had no missed appointments compared with 15.6% of control patients, and were 24.8 times more likely to not have a cancellation <24 hours before their appointment (P<.001). All navigated patients and their primary care providers received test results, and all follow-up recommendations were consistent with clinical guidelines compared with 82.4% of patients in the control group (P<.001).
Conclusions: PN appears to be effective for improving colonoscopy screening completion and quality in the disparate populations most in need of intervention. To the best of our knowledge, the results of the current study demonstrate some of the strongest evidence for the effectiveness of PN to date, and highlight its value for public health. Cancer 2017;123:3356-66. © 2017 American Cancer Society.
Keywords: colonoscopy; disparate populations; outcome assessment; patient adherence; patient navigation; public health.
© 2017 American Cancer Society.
Conflict of interest statement
CONFLICT OF INTEREST DISCLOSURES
Joanne Gersten and Lynn Butterly have received a grant from the Centers for Disease Control and Prevention for work performed as part of the current study. They also report that a copyright has been issued to the New Hampshire Colorectal Cancer Screening Program for the patient navigation model described in the current study.
Figures
Similar articles
-
Cost-effectiveness of a patient navigation intervention to increase colonoscopy screening among low-income adults in New Hampshire.Cancer. 2019 Feb 15;125(4):601-609. doi: 10.1002/cncr.31864. Epub 2018 Dec 12. Cancer. 2019. PMID: 30548480 Free PMC article.
-
Assessing the implementation of a patient navigation intervention for colonoscopy screening.BMC Health Serv Res. 2019 Nov 6;19(1):803. doi: 10.1186/s12913-019-4601-4. BMC Health Serv Res. 2019. PMID: 31694642 Free PMC article.
-
Economic assessment of patient navigation to colonoscopy-based colorectal cancer screening in the real-world setting at the University of Chicago Medical Center.Cancer. 2018 Nov 1;124(21):4137-4144. doi: 10.1002/cncr.31690. Epub 2018 Oct 25. Cancer. 2018. PMID: 30359474 Free PMC article.
-
Patient Navigation for Colonoscopy Completion: Results of an RCT.Am J Prev Med. 2017 Sep;53(3):363-372. doi: 10.1016/j.amepre.2017.05.010. Epub 2017 Jul 1. Am J Prev Med. 2017. PMID: 28676254 Free PMC article. Clinical Trial.
-
Evidence Brief: Comparative Effectiveness of Appointment Recall Reminder Procedures for Follow-up Appointments [Internet].Washington (DC): Department of Veterans Affairs (US); 2015 Jul. Washington (DC): Department of Veterans Affairs (US); 2015 Jul. PMID: 27606388 Free Books & Documents. Review.
Cited by
-
Reach and effectiveness of a centralized navigation program for patients with positive fecal immunochemical tests requiring follow-up colonoscopy.Prev Med Rep. 2023 Apr 17;34:102211. doi: 10.1016/j.pmedr.2023.102211. eCollection 2023 Aug. Prev Med Rep. 2023. PMID: 37214164 Free PMC article.
-
Associations between Missed Colonoscopy Appointments and Multiple Prior Adherence Behaviors in an Integrated Healthcare System: An Observational Study.J Gen Intern Med. 2024 Jan;39(1):36-44. doi: 10.1007/s11606-023-08355-5. Epub 2023 Aug 7. J Gen Intern Med. 2024. PMID: 37550443 Free PMC article.
-
Effectiveness of behavior change techniques to address barriers to follow-up colonoscopy: results from an online survey and randomized factorial experiment.Ann Behav Med. 2025 Jan 4;59(1):kaae083. doi: 10.1093/abm/kaae083. Ann Behav Med. 2025. PMID: 39739614 Free PMC article. Clinical Trial.
-
Primary Care Clinician Perspectives on Patient Navigation to Improve Postpartum Care for Patients with Low Income.Womens Health Rep (New Rochelle). 2022 Dec 15;3(1):1006-1015. doi: 10.1089/whr.2022.0064. eCollection 2022. Womens Health Rep (New Rochelle). 2022. PMID: 36636317 Free PMC article.
-
A qualitative process evaluation of a diabetes navigation program embedded in an endocrine specialty center in rural Appalachian Ohio.BMC Endocr Disord. 2018 Jul 27;18(1):50. doi: 10.1186/s12902-018-0278-7. BMC Endocr Disord. 2018. PMID: 30053846 Free PMC article.
References
-
- US Cancer Statistics Working Group. United States Cancer Statistics: 1999–2013 Incidence and Mortality Web-Based Report. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention, and National Cancer Institute; 2015. [Accessed July 6, 2016]. www.cdc.gov/uscs.
-
- Winawer SJ, Zauber AG, Ho MN, et al. Prevention of colorectal cancer by colonoscopic polypectomy. The National Polyp Study Workgroup. N Engl J Med. 1993;329:1977–1981. - PubMed
-
- US Preventive Services Task Force. [Accessed July 7, 2016];Final Recommendation Statement: Colorectal Cancer: Screening. 2008 Oct; http://www.uspreventiveservicestaskforce.org/Page/Document/Recommendatio... colorectal-cancer-screening.
-
- Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance System Survey Data. Atlanta, GA: US Department of Health and Human Services, Centers for Disease Control and Prevention; 2014. [Accessed January 27, 2016]. http://www.cdc.gov/brfss/index.html.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
