

Prognostic factors in hospitalized community-acquired pneumonia: a retrospective study of a prospective observational cohort
- PMID: 28464807
- PMCID: PMC5414343
- DOI: 10.1186/s12890-017-0424-4
Prognostic factors in hospitalized community-acquired pneumonia: a retrospective study of a prospective observational cohort
Abstract
Background: To date, only few studies have examined the prognostic factors of community-acquired pneumonia (CAP) defined according to the latest criteria, which excludes healthcare-associated pneumonia (HCAP). Therefore, we aimed to investigate the factors that affect prognosis, and evaluate the usefulness of existing pneumonia severity scores for predicting the prognosis of CAP.
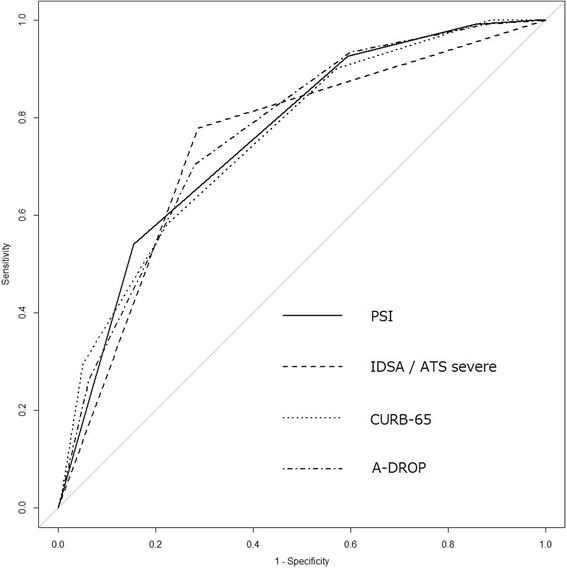
Methods: We retrospectively analyzed patients with CAP, excluding HCAP, who were enrolled prospectively between April 2007 and February 2016. Four patients who used macrolides other than azithromycin (AZM) were excluded. We used age, sex, comorbidities, laboratory findings and antimicrobial therapy as prognostic variables. The primary outcome was 30-day mortality and secondary outcome was ICU admission. We also performed receiver operating characteristic curve analysis of Pneumonia Severity Index (PSI), Infectious Diseases Society of America (IDSA)/American Thoracic Society (ATS) severe criteria, CURB-65 and A-DROP pneumonia severity scores.
Results: Among 1834 CAP patients, mean age was 73.5 ± 14.3 years; 1281 (69.8%) were men; and 30-day mortality was 6.7% (122/1834). In total, 1830 patients were analyzed. Multivariate analysis identified age [Odds Ratio (OR): 1.04, 95% Confidence Interval (CI): 1.02-1.07], chronic obstructive pulmonary disease (COPD) [OR: 1.77, 95% CI: 1.13-2.76], malignancy (OR: 2.25, 95% CI: 1.25-4.06), body temperature (OR: 0.81, 95% CI: 0.67-0.99), respiratory rate (OR: 1.04, 95% CI: 1.01-1.07), PaO2/FiO2 ≤ 250 (OR: 3.15, 95% CI: 1.93-5.14), Alb (OR: 0.27, 95% CI: 0.19-0.39), BUN (OR: 1.01, 95% CI: 1.00-1.02), and mechanical ventilation (OR: 2.99, 95% CI: 1.75-5.12) as prognostic factors. AZM and β-lactam combination therapy significantly reduced 30-day mortality (OR: 0.50, 95% CI: 0.26-0.97). Areas under the curve of PSI, IDSA/ATS severe criteria, CURB-65 and A-DROP were 0.759, 0.746, 0.754 and 0.764, respectively.
Conclusions: Increasing age, presence of COPD and malignancy as comorbidities, hypothermia, tachypnea, PaO2/FiO2 ratio ≤250 mmHg, low Alb level, high BUN level and mechanical ventilatory support predict a worse prognosis; AZM combination therapy should be considered for CAP, excluding HCAP. All four pneumonia severity scores are useful for assessing the severity of CAP defined by the latest criteria.
Trial registration: UMIN-CTR UMIN000004353 . Registered 7 October 2010. Retrospectively registered.
Keywords: Azithromycin; Combination therapy; Community-acquired pneumonia; Prognosis; Severity score.
Figures
References
-
- Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis. 2007;44(Suppl 2):S27–72. doi: 10.1086/511159. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
