

Primary extragenital endometrial stromal sarcoma of the lung: first reported case and review of literature
- PMID: 28464838
- PMCID: PMC5414122
- DOI: 10.1186/s13000-017-0627-2
Primary extragenital endometrial stromal sarcoma of the lung: first reported case and review of literature
Abstract
Background: Endometrial stromal sarcomas arising in extrauterine and extraovarian sites, in the absence of a primary uterine lesion are quite rare, especially in the absence of endometriosis. They usually present as an abdominal or pelvic mass lesion.
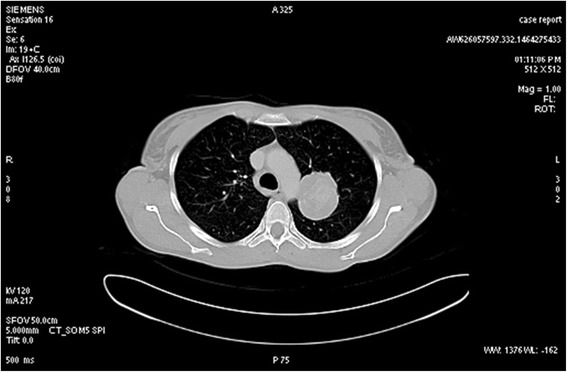
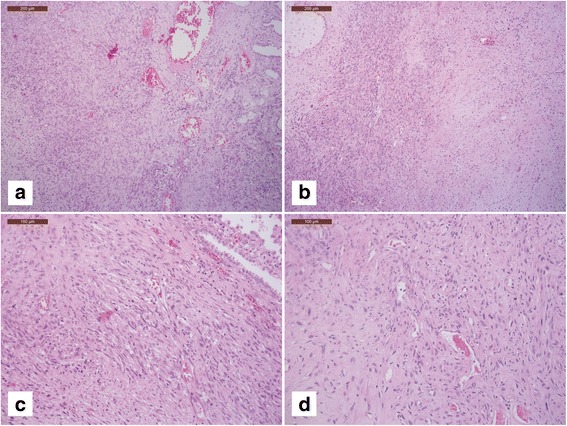
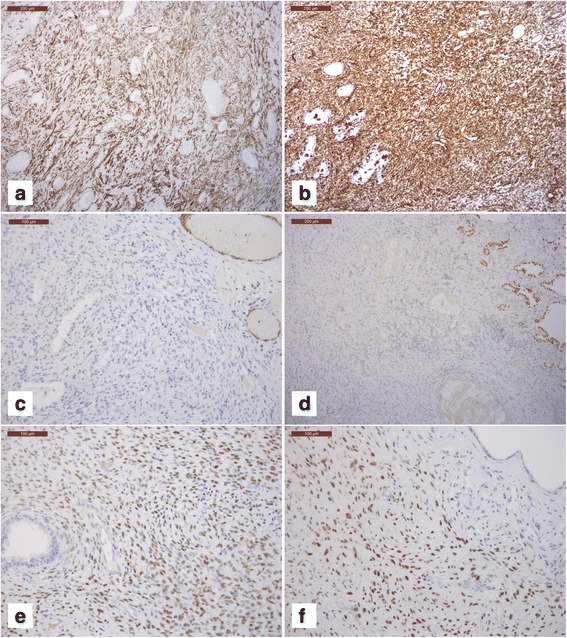
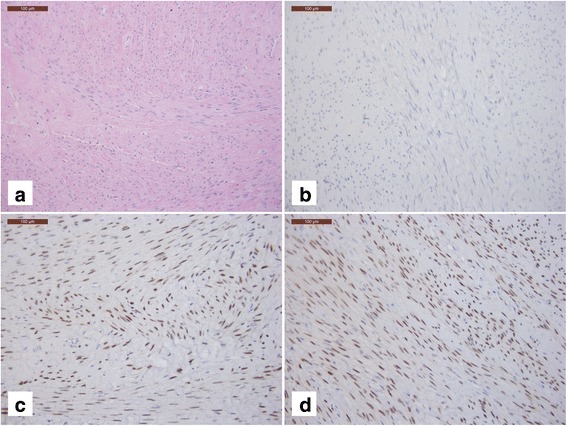
Case presentation: In 2007, a 45-year-old woman underwent total hysterectomy for in situ squamous cell carcinoma of the cervix. In 2014, an upper left pulmonary lobectomy was performed for a mass, which was provisionally diagnosed as primary carcinosarcoma of the lung. A second histological revision of the lung surgical specimen was performed in the Pathology Unit of our Institute. After extensive immunohistochemical analyses, the preferred diagnosis was spindle-cell sarcoma, consistent with high-grade extragenital endometrial stromal sarcoma (EESS). A review of all slides of the hysterectomy specimen confirms the original diagnosis: no evidence of stromal tumor was found. Afterwards, the patient developed multiple and metachronous pulmonary lesions and a scapular soft tissue mass, which showed the same morphophenotypic features of the first lung mass. The patient was treated with antiblastic therapy, surgical resection and radioablation, when appropriate. To date, the patient has no signs or symptoms.
Conclusions: The authors present the first case of primary EESS arising in the lung with no association with endometriosis published to date. Detailed clinical history and follow-up are also described. Moreover, extensive literature review is reported, along with differential diagnoses, immunohistochemical and molecular findings, pathogenetic hypotheses and treatment options. The knowledge of EESS potential extrauterine location and of its peculiar morphophenotypic aspects are required for a correct diagnosis, and for choosing the most suitable treatment.
Keywords: Case report; Extragenital endometrial stromal sarcoma; Immunohistochemistry; Lung.
Figures
References
-
- Kurman R, Carcangiu ML, Herrington C, et al. WHO classification of tumours of female reproductive organs. IARC WHO Classification of Tumours, No 6. Lyon: IARC press; 2014.
-
- Ferraro LR, Hetz H, Carter H. Malignant endometriosis; pelvic endometriosis complicated by polypoid endometrioma of the colon and endometriotic sarcoma; report of a case and review of the literature. Obstet Gynecol. 1956;7(1):32–9. - PubMed
-
- Berkowitz RS, Ehrmann RL, Knapp RC. Endometrial stromal sarcoma arising from vaginal endometriosis. Obstet Gynecol. 1978;51(1 Suppl):34s–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
