

Invasive meningococcal disease in the Veneto region of Italy: a capture-recapture analysis for assessing the effectiveness of an integrated surveillance system
- PMID: 28465304
- PMCID: PMC5623379
- DOI: 10.1136/bmjopen-2016-012478
Invasive meningococcal disease in the Veneto region of Italy: a capture-recapture analysis for assessing the effectiveness of an integrated surveillance system
Abstract
Background: Epidemiology of Neisseria meningitidis has been changing since the introduction of universal vaccination programmes against meningococcal serogroup C (MenC) and meningococcal serogroup B (MenB) has now become dominant. This study aimed to analyse the cases reported in institutional data recording systems to estimate the burden of invasive meningococcal diseases (IMDs) and assess the effectiveness of surveillance in Veneto region (Italy).
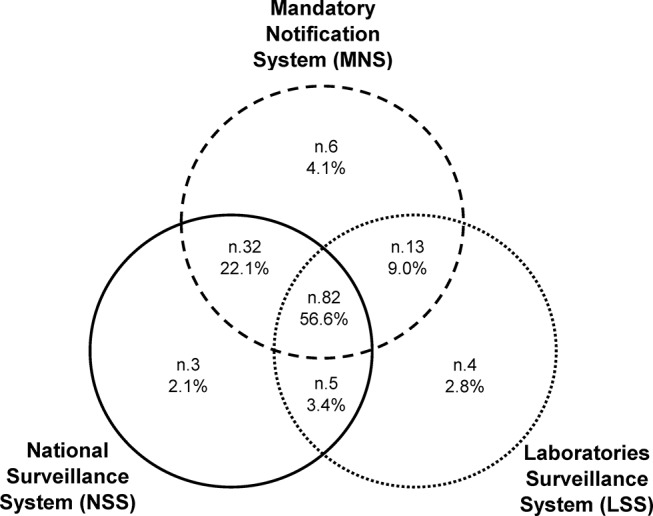
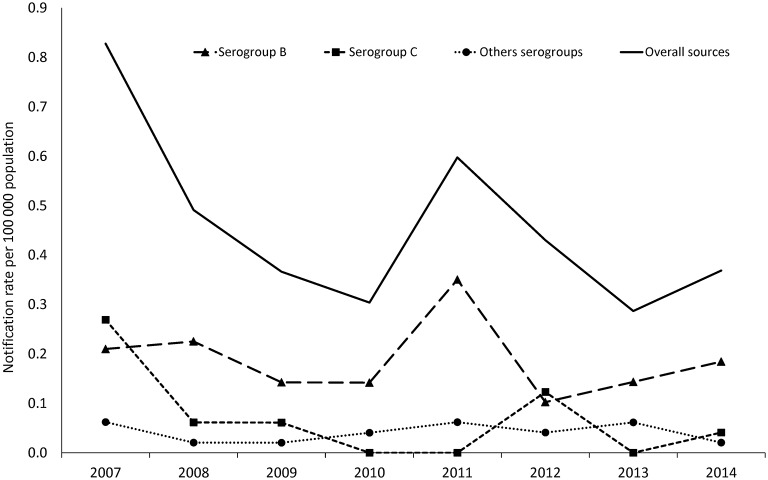
Methods: Analysis was performed from 2007 to 2014 on data recorded in different systems: Mandatory Notification System, National Surveillance of Invasive Bacterial Diseases System and Laboratories Surveillance System (LSS), which were pooled into a combined surveillance system (CSS) and hospital discharge records (HDRs). A capture-recapture method was used and completeness of each source estimated. Number of cases with IMD by source of information and year, incidence of IMD by age group, case fatality rate (CFR) and distribution of meningococcal serogroups by year were also analysed.
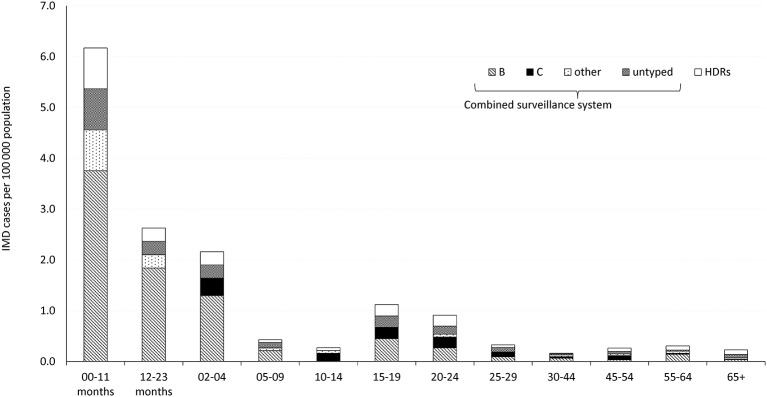
Results: Combining the four data systems enabled the identification of 179 confirmed cases with IMD, achieving an overall sensitivity of 94.7% (95% CI: 90.8% to 98.8%), while it was 76.7% (95% CI: 73.6% to 80.1%) for CSS and 77.2% (95% CI: 74.1% to 80.6%) for HDRs. Typing of isolates was done in 80% of cases, and 95.2% of the typed cases were provided by LSS. Serogroup B was confirmed in 50.3% of cases. The estimated IMD notification rate (cases with IMD diagnosed and reported to the surveillance systems) was 0.48/100 000 population, and incidence peaked at 6.2/100 000 in children aged <1 year old (60.9% due to MenB), and increased slightly in the age group between 15 and 19 years (1.1/100 000). A CFR of 14% was recorded (8.7% in paediatric age).
Conclusions: Quality of surveillance systems relies on case ascertainment based on serological characterisation of the circulating strains by microbiology laboratories. All available sources should be routinely combined to improve the epidemiology of IMD and the information used by public health departments to conduct timely preventive measures.
Keywords: laboratory surveillance data; meningococcal disease; sensitivity; surveillance systems.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2017. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Epidemiological and Molecular Characterization of Invasive Meningococcal Disease in Italy, 2008/09-2012/13.PLoS One. 2015 Oct 7;10(10):e0139376. doi: 10.1371/journal.pone.0139376. eCollection 2015. PLoS One. 2015. PMID: 26445461 Free PMC article.
-
Culture-Confirmed Invasive Meningococcal Disease in Canada, 2010 to 2014: Characterization of Serogroup B Neisseria meningitidis Strains and Their Predicted Coverage by the 4CMenB Vaccine.mSphere. 2020 Mar 4;5(2):e00883-19. doi: 10.1128/mSphere.00883-19. mSphere. 2020. PMID: 32132156 Free PMC article.
-
Reduction in Neisseria meningitidis infection in Italy after Meningococcal C conjugate vaccine introduction: A time trend analysis of 1994-2012 series.Hum Vaccin Immunother. 2016;12(2):467-73. doi: 10.1080/21645515.2015.1078951. Hum Vaccin Immunother. 2016. PMID: 26308192 Free PMC article.
-
A Review of the Epidemiology of Invasive Meningococcal Disease and Vaccination Strategies in North Africa.Int J Infect Dis. 2021 Mar;104:189-197. doi: 10.1016/j.ijid.2020.11.162. Epub 2020 Nov 20. Int J Infect Dis. 2021. PMID: 33227521 Review.
-
Epidemiological burden of meningococcal disease in Brazil: A systematic literature review and database analysis.Int J Infect Dis. 2019 Mar;80:137-146. doi: 10.1016/j.ijid.2019.01.009. Epub 2019 Jan 11. Int J Infect Dis. 2019. PMID: 30641200
Cited by
-
Evaluation of the national surveillance system for invasive meningococcal disease, Italy, 2015-2018.PLoS One. 2021 Jan 8;16(1):e0244889. doi: 10.1371/journal.pone.0244889. eCollection 2021. PLoS One. 2021. PMID: 33417620 Free PMC article.
-
Surveillance of Pediatric Invasive Bacterial Diseases in the Veneto Region: Epidemiological Trends and Outcomes over 17 Years (2007-2023).Vaccines (Basel). 2025 Feb 24;13(3):230. doi: 10.3390/vaccines13030230. Vaccines (Basel). 2025. PMID: 40266085 Free PMC article.
-
Invasive Pneumococcal Disease in Tuscany Region, Italy, 2016-2017: Integrating Multiple Data Sources to Investigate Underreporting.Int J Environ Res Public Health. 2020 Oct 19;17(20):7581. doi: 10.3390/ijerph17207581. Int J Environ Res Public Health. 2020. PMID: 33086480 Free PMC article.
-
[Health Technology Assessment of meningococcal B vaccine (Trumenba®) in adolescent in Italy].J Prev Med Hyg. 2019 Dec 19;60(3 Suppl 2):E1-E94. doi: 10.15167/2421-4248/jpmh2019.60.3s2. eCollection 2019 Dec. J Prev Med Hyg. 2019. PMID: 32047867 Free PMC article. Italian. No abstract available.
-
Invasive meningococcal disease in Italy: from analysis of national data to an evidence-based vaccination strategy.J Prev Med Hyg. 2020 Jul 4;61(2):E152-E161. doi: 10.15167/2421-4248/jpmh2020.61.2.1589. eCollection 2020 Jun. J Prev Med Hyg. 2020. PMID: 32802999 Free PMC article.
References
-
- Greenwood BM. The epidemiology of acute bacterial meningitis in tropical Africa : Williams JD, Burnie J, Bacterial meningitis. London: Academic Press, 1987:61–91.
-
- Centers for Disease Control. Active bacterial corecore surveillance (ABCs) report emerging infections program network Neisseria meningitidis, 2009. Available on http://www.cdc.gov/abcs/reports-findings/survreports/mening09.pdf (accessed 18th Feb 2016).
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases