

Treatment Patterns and Outcomes in Patients with Varicose Veins
- PMID: 28465773
- PMCID: PMC5394556
Treatment Patterns and Outcomes in Patients with Varicose Veins
Abstract
Background: Approximately 24% of adults in the United States have visible varicose veins, and an estimated 6% have evidence of advanced chronic venous disease. The majority of individuals with varicose veins seek treatment because of symptoms, such as aching, throbbing, fatigue, pruritus, ankle swelling, and tenderness, rather than cosmetic reasons. Furthermore, varicose veins are a manifestation of chronic venous insufficiency, which can progress to leg pain, leg edema, chronic skin changes, and nonhealing ulcers.
Objective: To assess varicose vein treatment patterns and their corresponding outcomes, including additional treatment rates, disease progression to new ulcers, and associated costs from a US perspective.
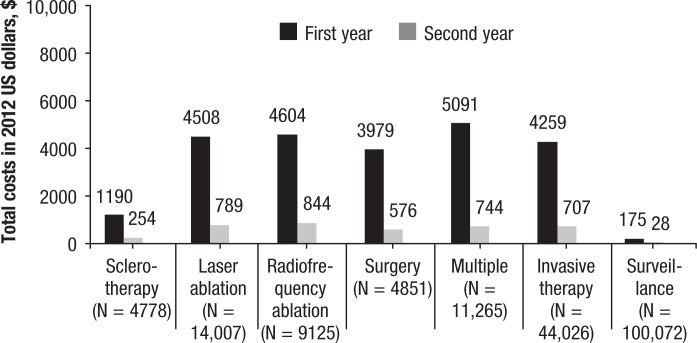
Methods: We conducted a retrospective claims database study using data from the Truven Health MarketScan database. Adults who were newly diagnosed with varicose veins between January 1, 2008, and June 30, 2010, and met the study inclusion criteria were eligible to participate and were divided into 6 cohorts based on the type of first or initial therapy they received after the index diagnosis date, including surveillance and compression therapy, surgery, laser ablation, radiofrequency ablation, sclerotherapy, or multiple therapies. The patients were followed for 2 years after the index diagnosis date to assess their treatment patterns and outcomes.
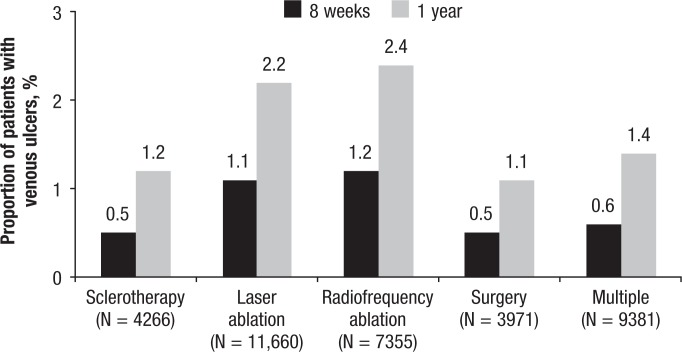
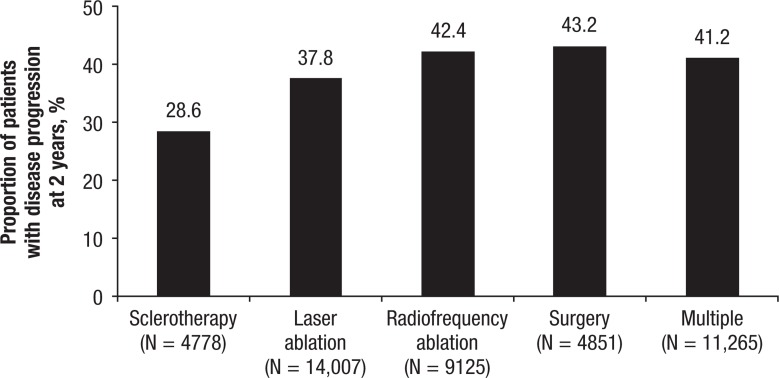
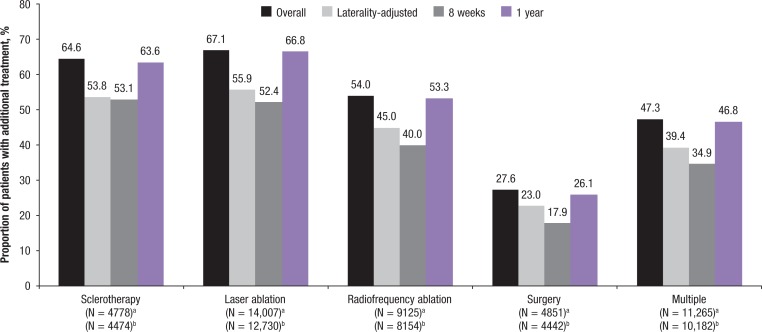
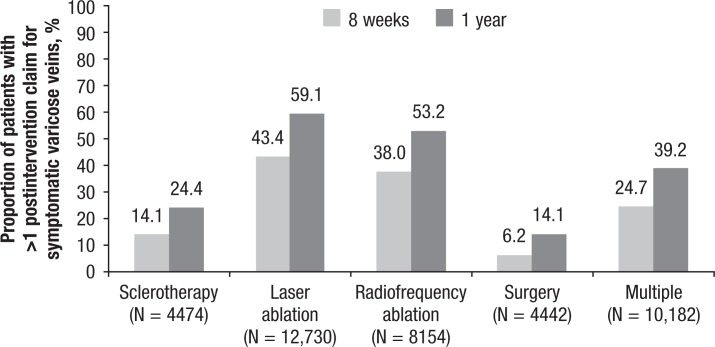
Results: A total of 144,098 patients met the study criteria. Of these patients, 100,072 (69.5%) were under surveillance for disease progression and/or received compression therapy; 14,007 (9.7%) received laser ablation; 9125 (6.3%) received radiofrequency ablation; 4778 (3.3%) received sclerotherapy; 4851 (3.4%) had surgery; and 11,265 (7.8%) received multiple therapies. During the 2-year follow-up period, among patients receiving interventional treatment, 54.7% of patients received additional interventional treatment (either with the same mode or a different mode from the initial treatment); 30.1% had >1 postintervention claim for symptomatic varicose veins (not including additional procedures) at 8 weeks; and 44.2% had >1 postintervention claim for symptomatic varicose veins at 1 year after the initial interventional therapy.
Conclusions: A majority of the patients in the study received conservative management. For patients receiving interventional therapy, the outcomes varied based on the treatment cohort. The surgery cohort was associated with the most favorable outcome regarding the need for additional treatment and evidence of postintervention claims for symptomatic varicose veins, followed by the multiple therapies cohort. A better understanding of these treatment outcomes in the real-world setting may affect new strategies to improve the management of patients with varicose veins.
Keywords: conservative therapy; cost; interventional therapy; observational study; outcomes; surveillance; treatment patterns; varicose veins.
Figures

References
-
- Kaplan RM, Criqui MH, Denenberg JO, et al. Quality of life in patients with chronic venous disease: San Diego population study. J Vasc Surg. 2003; 37: 1047–1053. - PubMed
-
- Gloviczki P, Comerota AJ, Dalsing MC, et al; for the Society for Vascular Surgery; American Venous Forum. The care of patients with varicose veins and associated chronic venous diseases: clinical practice guidelines of the Society for Vascular Surgery and the American Venous Forum. J Vasc Surg. 2011; 53 (5 suppl): 2S–48S. - PubMed
-
- Labropoulos N, Leon L, Kwon S, et al. Study of the venous reflux progression. J Vasc Surg. 2005; 41: 291–295. - PubMed
-
- Bergan JJ, Schmid-Schönbein GW, Smith PD, et al. Chronic venous disease. N Engl J Med. 2006; 355: 488–498. - PubMed
-
- Kumar RN, Gupchup GV, Dodd MA, et al. Direct health care costs of 4 common skin ulcers in New Mexico Medicaid fee-for-service patients. Adv Skin Wound Care. 2004; 17: 143–149. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous