

High-flow nasal cannula to prevent postextubation respiratory failure in high-risk non-hypercapnic patients: a randomized multicenter trial
- PMID: 28466461
- PMCID: PMC5413462
- DOI: 10.1186/s13613-017-0270-9
High-flow nasal cannula to prevent postextubation respiratory failure in high-risk non-hypercapnic patients: a randomized multicenter trial
Abstract
Background: Extubation failure is associated with increased morbidity and mortality, but cannot be safely predicted or avoided. High-flow nasal cannula (HFNC) prevents postextubation respiratory failure in low-risk patients.
Objective: To demonstrate that HFNC reduces postextubation respiratory failure in high-risk non-hypercapnic patients compared with conventional oxygen.
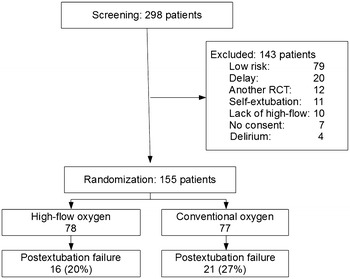
Methods: Randomized, controlled multicenter trial in patients who passed a spontaneous breathing trial. We enrolled patients meeting criteria for high-risk of failure to randomly receive HFNC or conventional oxygen for 24 h after extubation. Primary outcome was respiratory failure within 72-h postextubation. Secondary outcomes were reintubation, intensive care unit (ICU) and hospital lengths of stay, and mortality. Statistical analysis included multiple logistic regression models.
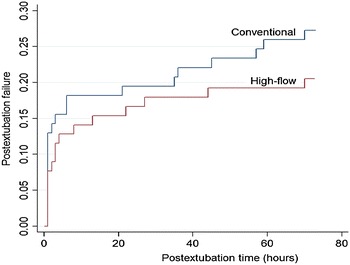
Results: The study was stopped due to low recruitment after 155 patients were enrolled (78 received high-flow and 77 received conventional oxygen). Groups were similar at enrollment, and all patients tolerated 24-h HFNC. Postextubation respiratory failure developed in 16 (20%) HFNC patients and in 21 (27%) conventional patients [OR 0.69 (0.31-1.54), p = 0.2]. Reintubation was needed in 9 (11%) HFNC patients and in 12 (16%) conventional patients [OR 0.71 (0.25-1.95), p = 0.5]. No difference was found in ICU or hospital length of stay, or mortality. Logistic regression models suggested HFNC [OR 0.43 (0.18-0.99), p = 0.04] and cancer [OR 2.87 (1.04-7.91), p = 0.04] may be independently associated with postextubation respiratory failure.
Conclusion: Our study is inconclusive as to a potential benefit of HFNC over conventional oxygen to prevent occurrence of respiratory failure in non-hypercapnic patients at high risk for extubation failure. Registered at Clinicaltrials.gov NCT01820507.
Keywords: High-flow oxygen; Mechanical ventilation; Reintubation; Weaning.
Figures
References
-
- Esteban A, Frutos-Vivar F, Muriel A, Ferguson ND, Peñuelas O, Abraira V, Raymondos K, Rios F, Nin N, Apezteguía C, Violi DA, Thille AW, Brochard L, González M, Villagomez AJ, Hurtado J, Davies AR, Du B, Maggiore SM, Pelosi P, Soto L, Tomicic V, D’Empaire G, Matamis D, Abroug F, Moreno RP, Soares MA, Arabi Y, Sandi F, Jibaja M, Amin P, Koh Y, Kuiper MA, Bülow HH, Zeggwagh AA, Anzueto A. Evolution of mortality over time in patients receiving mechanical ventilation. Am J Respir Crit Care Med. 2013;188:220–230. doi: 10.1164/rccm.201212-2169OC. - DOI - PubMed
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
