

Gaps and barriers in the control of blood glucose in people with type 2 diabetes
- PMID: 28467203
- PMCID: PMC5418936
- DOI: 10.1177/1479164116679775
Gaps and barriers in the control of blood glucose in people with type 2 diabetes
Abstract
Background: Glycaemic control is suboptimal in a large proportion of people with type 2 diabetes who are consequently at an increased and avoidable risk of potentially severe complications. We sought to explore attitudes and practices among healthcare professionals that may contribute to suboptimal glycaemic control through a review of recent relevant publications in the scientific literature.
Methods: An electronic search of the PubMed database was performed to identify relevant publications from January 2011 to July 2015. The electronic search was complemented by a manual search of abstracts from key diabetes conferences in 2014/2015 available online.
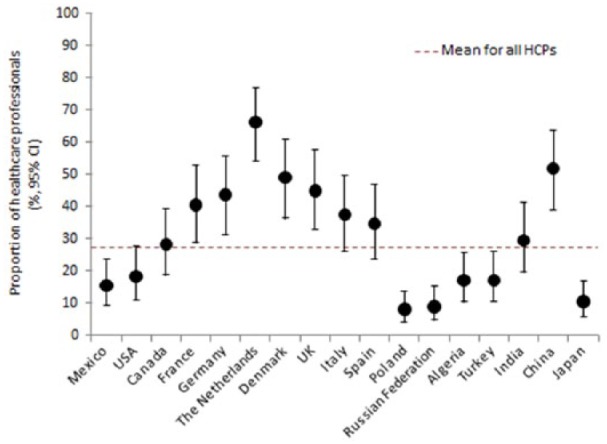
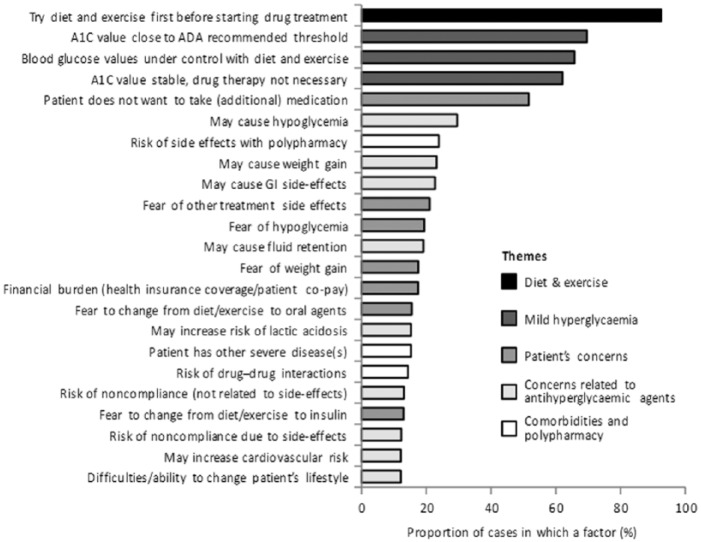
Results: Recently published data indicate that glycaemic control is suboptimal in a substantial proportion (typically 40%-60%) of people with diabetes. This is the case across geographic regions and in both low- and higher-income countries. Therapeutic inertia appears to be an important contributor to poor glycaemic control in up to half of people with type 2 diabetes. In particular, prescribers are often willing to tolerate extended periods of 'mild' hyperglycaemia as well as having low expectations for their patients. There are often delays of 3 years or longer in initiating or intensifying glucose-lowering therapy when needed.
Conclusion: Many people with type 2 diabetes are failed by current management, with approximately half not achieving or maintaining appropriate target blood glucose levels, leaving these patients at increased and avoidable risk of serious complications. Review criteria: The methodology of this review article is detailed in the 'Methods' section.
Keywords: Diabetes mellitus; clinical inertia; glycaemic control; review; surveys; type 2.
Conflict of interest statement
Figures
References
-
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33). Lancet 1998; 352: 837–853. - PubMed
-
- Holman RR, Paul SK, Bethel MA, et al. 10-year follow-up of intensive glucose control in type 2 diabetes. N Engl J Med 2008; 359: 1577–1589. - PubMed
-
- Writing Team for the Diabetes Control and Complications Trial/Epidemiology of Diabetes Interventions and Complications Research Group. Sustained effect of intensive treatment of type 1 diabetes mellitus on development and progression of diabetic nephropathy: the Epidemiology of Diabetes Interventions and Complications (EDIC) study. JAMA 2003; 290: 2159–2167. - PMC - PubMed
-
- Aschner PJ, Ruiz AJ. Metabolic memory for vascular disease in diabetes. Diabetes Technol Ther 2012; 14(Suppl. 1): S68–S74. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
