

Association of the Modified Frailty Index With 30-Day Surgical Readmission
- PMID: 28467535
- PMCID: PMC5710500
- DOI: 10.1001/jamasurg.2017.1025
Association of the Modified Frailty Index With 30-Day Surgical Readmission
Abstract
Importance: Frail patients are known to have poor perioperative outcomes. There is a paucity of literature investigating how the Modified Frailty Index (mFI), a validated measure of frailty, is associated with unplanned readmission among military veterans following surgery.
Objective: To understand the association between frailty and 30-day postoperative unplanned readmission.
Design, setting, and participants: A retrospective cohort study was conducted among adult patients who underwent surgery and were discharged alive from Veterans Affairs hospitals for orthopedic, general, and vascular conditions between October 1, 2007, and September 30, 2014, with a postoperative length of stay between 2 and 30 days.
Exposure: Frailty, as calculated by the 11 variables on the mFI.
Main outcomes and measures: The primary outcome of interest is 30-day unplanned readmission. Secondary outcomes included any 30-day predischarge or postdischarge complication, 30-day postdischarge mortality, and 30-day emergency department visit.
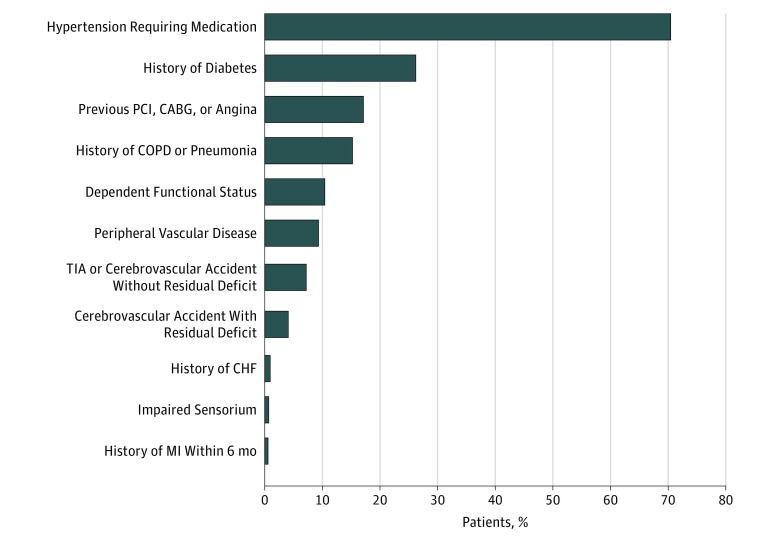
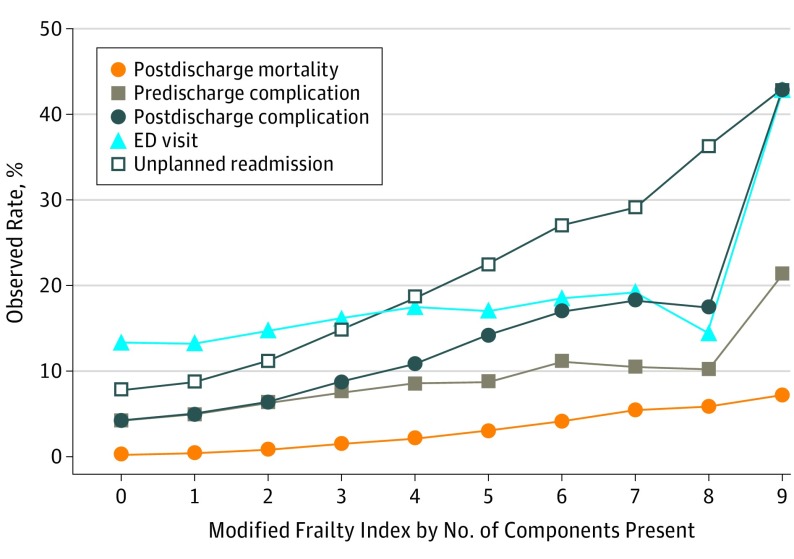
Results: The study sample included 236 957 surgical procedures (among 223 877 men and 13 080 women; mean [SD] age, 64.0 [11.3] years) from high-volume surgical specialties: 101 348 procedures (42.8%) in orthopedic surgery, 92 808 procedures (39.2%) in general surgery, and 42 801 procedures (18.1%) in vascular surgery. The mFI was associated with readmission (odds ratio [OR], 1.11; 95% CI, 1.10-1.12; R2 = 10.3%; C statistic, 0.71). Unadjusted rates of overall 30-day readmission (26 262 [11.1%]), postdischarge emergency department visit (34 204 [14.4%]), any predischarge (13 855 [5.9%]) or postdischarge (14 836 [6.3%]) complication, and postdischarge mortality (1985 [0.8%]) varied by frailty in a dose-dependent fashion. In analysis by individual mFI components using Harrell ranking, impaired functional status, identified as nonindependent functional status (OR, 1.16; 95% CI, 1.11-1.21; P < .01) or having a residual deficit from a prior cerebrovascular accident (OR, 1.17; 95% CI, 1.11-1.22; P < .01), contributed most to the ability of the mFI to anticipate readmission compared with the other components. Acutely impaired sensorium (OR, 1.12; 95% CI, 0.99-1.27; P = .08) and history of a myocardial infarction within 6 months (OR, 0.93; 95% CI, 0.81-1.06; P = .28) were not significantly associated with readmission.
Conclusions and relevance: The mFI is associated with poor surgical outcomes, including readmission, primarily due to impaired functional status. Targeting potentially modifiable aspects of frailty preoperatively, such as improving functional status, may improve perioperative outcomes and decrease readmissions.
Conflict of interest statement
Figures
Comment in
-
Frailty-Going From Measurement to Action.JAMA Surg. 2017 Aug 1;152(8):757-758. doi: 10.1001/jamasurg.2017.1050. JAMA Surg. 2017. PMID: 28467521 No abstract available.
References
-
- McIsaac DI, Bryson GL, van Walraven C. Association of frailty and 1-year postoperative mortality following major elective noncardiac surgery: a population-based cohort study. JAMA Surg. 2016;151(6):538-545. - PubMed
-
- Buigues C, Juarros-Folgado P, Fernández-Garrido J, Navarro-Martínez R, Cauli O. Frailty syndrome and pre-operative risk evaluation: a systematic review. Arch Gerontol Geriatr. 2015;61(3):309-321. - PubMed
-
- Revenig LM, Canter DJ, Taylor MD, et al. Too frail for surgery? initial results of a large multidisciplinary prospective study examining preoperative variables predictive of poor surgical outcomes. J Am Coll Surg. 2013;217(4):665-670.e1. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
