

A systematic review and meta-analysis of individual patient data on the impact of the BIM deletion polymorphism on treatment outcomes in epidermal growth factor receptor mutant lung cancer
- PMID: 28467813
- PMCID: PMC5522319
- DOI: 10.18632/oncotarget.17102
A systematic review and meta-analysis of individual patient data on the impact of the BIM deletion polymorphism on treatment outcomes in epidermal growth factor receptor mutant lung cancer
Abstract
Background: A germline deletion in the BIM (BCL2L11) gene has been shown to impair the apoptotic response to tyrosine kinase inhibitors (TKIs) in vitro but its association with poor outcomes in TKI-treated non-small cell lung cancer (NSCLC) patients remains unclear. We conducted a systematic review and meta-analysis on both aggregate and individual patient data to address this issue.
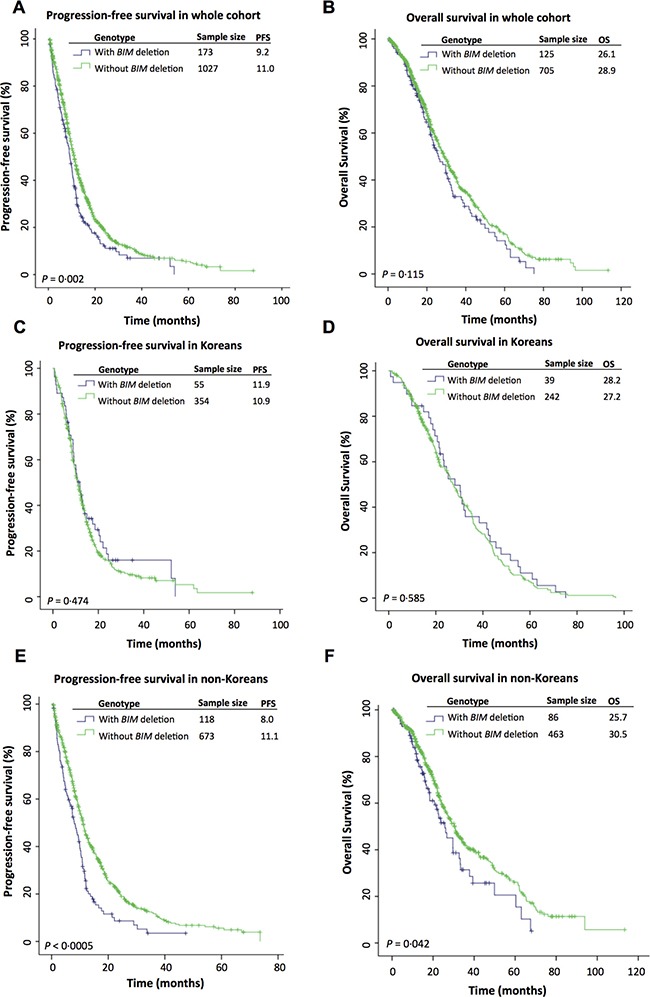
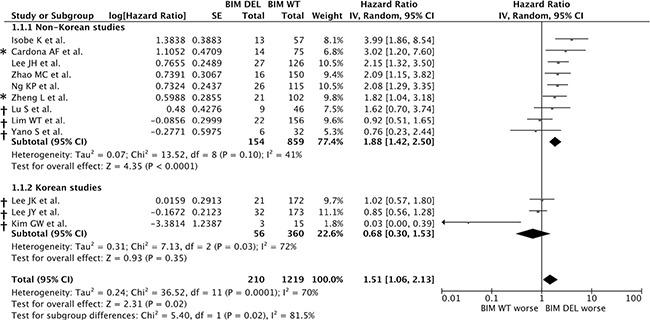
Results: In an aggregate data meta-analysis (n = 1429), the BIM deletion was associated with inferior PFS (HR = 1.51, 95%CI = 1.06-2.13, P = 0.02). Using individual patient data (n = 1200), we found a significant interaction between the deletion and ethnicity. Amongst non-Koreans, the deletion was an independent predictor of shorter PFS (Chinese: HR = 1.607, 95%CI = 1.251-2.065, P = 0.0002; Japanese: HR = 2.636, 95%CI = 1.603-4.335, P = 0.0001), and OS (HR = 1.457, 95% CI = 1.063-1.997, P = 0.019). In Kaplan-Meier analyses, the BIM deletion was associated with shorter survival in non-Koreans (PFS: 8.0 months v 11.1 months, P < 0.0005; OS: 25.7 v 30.0 months, P = 0.042). In Koreans, the BIM deletion was not predictive of PFS or OS.
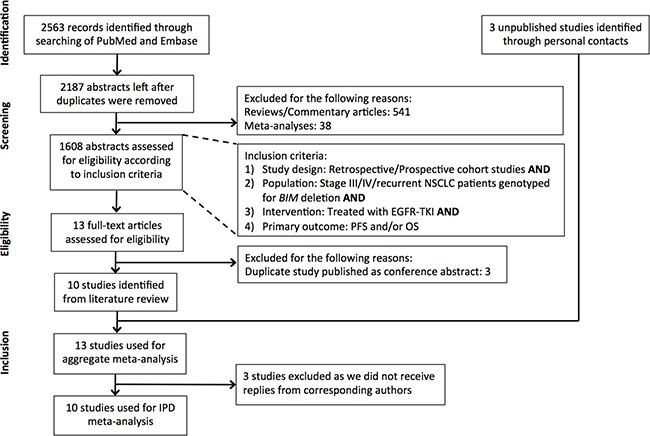
Materials and methods: 10 published and 3 unpublished studies that reported survival outcomes in NSCLC patients stratified according to BIM deletion were identified from PubMed and Embase. Summary risk estimates were calculated from aggregate patient data using a random-effects model. For individual patient data, Kaplan-Meier analyses were supported by multivariate Cox regression to estimate hazard ratios (HRs) for PFS and OS.
Conclusions: In selected populations, the BIM deletion is a significant predictor of shorter PFS and OS on EGFR-TKIs. Further studies to determine its effect on response to other BIM-dependent therapeutic agents are needed, so that alternative treatment strategies may be devised.
Keywords: BIM; drug resistance; lung cancer; polymorphism; tyrosine kinase inhibitor.
Conflict of interest statement
We declare no relevant competing interests.
Figures
References
-
- Pao W, Miller V, Zakowski M, Doherty J, Politi K, Sarkaria I, Singh B, Heelan R, Rusch V, Fulton L, Mardis E, Kupfer D, Wilson R, et al. EGF receptor gene mutations are common in lung cancers from “never smokers” and are associated with sensitivity of tumors to gefitinib and erlotinib. Proc Natl Acad Sci USA. 2004;101:13306–13311. - PMC - PubMed
-
- Lynch TJ, Bell DW, Sordella R, Gurubhagavatula S, Okimoto RA, Brannigan BW, Harris PL, Haserlat SM, Supko JG, Haluska FG, Louis DN, Christiani DC, Settleman J, et al. Activating mutations in the epidermal growth factor receptor underlying responsiveness of non-small-cell lung cancer to gefitinib. N Engl J Med. 2004;350:2129–2139. - PubMed
-
- Paez JG, Janne PA, Lee JC, Tracy S, Greulich H, Gabriel S, Herman P, Kaye FJ, Lindeman N, Boggon TJ, Naoki K, Sasaki H, Fujii Y, et al. EGFR mutations in lung cancer: correlation with clinical response to gefitinib therapy. Science. 2004;304:1497–1500. - PubMed
-
- Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, Saijo N, Sunpaweravong P, Han B, Margono B, Ichinose Y, Nishiwaki Y, Ohe Y, Yang JJ, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009;361:947–957. - PubMed
-
- Rosell R, Carcereny E, Gervais R, Vergnenegre A, Massuti B, Felip E, Palmero R, Garcia-Gomez R, Pallares C, Sanchez JM, Porta R, Cobo M, Garrido P, et al. Erlotinib versus standard chemotherapy as first-line treatment for European patients with advanced EGFR mutation-positive non-small-cell lung cancer (EURTAC): a multicentre, open-label, randomised phase 3 trial. Lancet Oncol. 2012;13:239–246. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
