

Teprotumumab for Thyroid-Associated Ophthalmopathy
- PMID: 28467880
- PMCID: PMC5718164
- DOI: 10.1056/NEJMoa1614949
Teprotumumab for Thyroid-Associated Ophthalmopathy
Abstract
Background: Thyroid-associated ophthalmopathy, a condition commonly associated with Graves' disease, remains inadequately treated. Current medical therapies, which primarily consist of glucocorticoids, have limited efficacy and present safety concerns. Inhibition of the insulin-like growth factor I receptor (IGF-IR) is a new therapeutic strategy to attenuate the underlying autoimmune pathogenesis of ophthalmopathy.
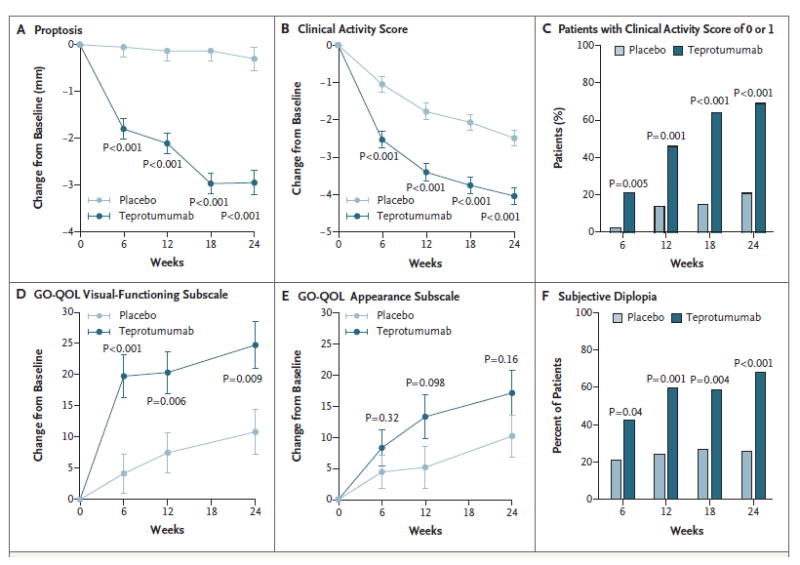
Methods: We conducted a multicenter, double-masked, randomized, placebo-controlled trial to determine the efficacy and safety of teprotumumab, a human monoclonal antibody inhibitor of IGF-IR, in patients with active, moderate-to-severe ophthalmopathy. A total of 88 patients were randomly assigned to receive placebo or active drug administered intravenously once every 3 weeks for a total of eight infusions. The primary end point was the response in the study eye. This response was defined as a reduction of 2 points or more in the Clinical Activity Score (scores range from 0 to 7, with a score of ≥3 indicating active thyroid-associated ophthalmopathy) and a reduction of 2 mm or more in proptosis at week 24. Secondary end points, measured as continuous variables, included proptosis, the Clinical Activity Score, and results on the Graves' ophthalmopathy-specific quality-of-life questionnaire. Adverse events were assessed.
Results: In the intention-to-treat population, 29 of 42 patients who received teprotumumab (69%), as compared with 9 of 45 patients who received placebo (20%), had a response at week 24 (P<0.001). Therapeutic effects were rapid; at week 6, a total of 18 of 42 patients in the teprotumumab group (43%) and 2 of 45 patients in the placebo group (4%) had a response (P<0.001). Differences between the groups increased at subsequent time points. The only drug-related adverse event was hyperglycemia in patients with diabetes; this event was controlled by adjusting medication for diabetes.
Conclusions: In patients with active ophthalmopathy, teprotumumab was more effective than placebo in reducing proptosis and the Clinical Activity Score. (Funded by River Vision Development and others; ClinicalTrials.gov number, NCT01868997 .).
Figures

Comment in
-
Thyroid disease: Potential new therapy for ophthalmopathy.Nat Rev Endocrinol. 2017 Jul;13(7):377. doi: 10.1038/nrendo.2017.67. Epub 2017 May 19. Nat Rev Endocrinol. 2017. PMID: 28524170 No abstract available.
-
Teprotumumab: a new avenue for the management of moderate-to-severe and active Graves' orbitopathy?J Endocrinol Invest. 2017 Aug;40(8):885-887. doi: 10.1007/s40618-017-0717-8. Epub 2017 Jun 20. J Endocrinol Invest. 2017. PMID: 28634704 No abstract available.
-
New antibody-based therapies for thyroid-associated ophthalmopathy.Surv Ophthalmol. 2018 May-Jun;63(3):447. doi: 10.1016/j.survophthal.2017.12.004. Epub 2017 Dec 15. Surv Ophthalmol. 2018. PMID: 29248534 No abstract available.
References
-
- Smith TJ, Hegedüs L. Graves’ disease. N Engl J Med. 2016;375:1552–65. - PubMed
-
- Sandler HM, Rubenstein JH, Fowble BL, Sergott RC, Savino PJ, Bosley TM. Results of radiotherapy for thyroid ophthalmopathy. Int J Radiat Oncol Biol Phys. 1989;17:823–7. - PubMed
-
- Bartalena L, Krassas GE, Wiersinga W, et al. Efficacy and safety of three different cumulative doses of intravenous methylprednisolone for moderate to severe and active Graves’ orbitopathy. J Clin Endocrinol Metab. 2012;97:4454–63. - PubMed
-
- Zang S, Ponto KA, Kahaly GJ. Clinical review: intravenous glucocorticoids for Graves’ orbitopathy: efficacy and morbidity. J Clin Endocrinol Metab. 2011;96:320–32. - PubMed
-
- Sisti E, Coco B, Menconi F, et al. Intravenous glucocorticoid therapy for Graves’ ophthalmopathy and acute liver damage: an epidemiological study. Eur J Endocrinol. 2015;172:269–76. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Other Literature Sources