

Immune Tolerant Chronic Hepatitis B: The Unrecognized Risks
- PMID: 28468285
- PMCID: PMC5454409
- DOI: 10.3390/v9050096
Immune Tolerant Chronic Hepatitis B: The Unrecognized Risks
Abstract
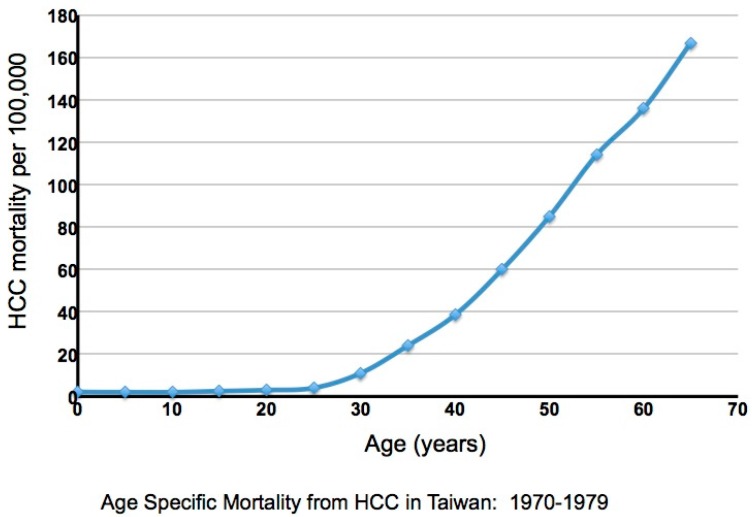
Chronic infection with hepatitis B virus (HBV) progresses through multiple phases, including immune tolerant, immune active, immune control, and, in a subset of patients who achieve immune control, reactivation. The first, the immune tolerant phase, is considered to be prolonged in duration but essentially benign in nature, lacking long-term consequences, and thus not recommended for antiviral therapy. This review challenges the notion that the immune tolerant phase is truly benign and considers the possibility that events during this phase may contribute significantly to cirrhosis, hepatocellular carcinoma (HCC), and the premature death of 25% of HBV carriers worldwide. Thus, earlier treatment than recommended by current guidelines should be considered. Low therapeutic coverage exacerbated by restrictive treatment guidelines may facilitate disease progression in many patients but also increase the risk of neonatal and horizontal transmission from untreated mothers to their children. While a prophylactic vaccine exists, there are many areas worldwide where the treatment of adults and the delivery of an effective vaccination course to newborns present difficult challenges.
Keywords: cirrhosis; hepatitis B; hepatocellular carcinoma; immune tolerant; inflammation; vaccine.
Conflict of interest statement
(PTFK) has received educational grants from Gilead Sciences. In addition, he has acted as a consultant for Gilead, Jannsen, BMS and Roche. Speaker bureau: Gilead, BMS and Roche. A.B. declares the following relationship with commercial entities developing therapeutics for HBV treatment: A.B. collaborates and receives research support from Gilead Sciences to test the effect of HBV antigens on immune cell function. In addition, he has acted as a consultant and served on the advisory boards of Gilead Sciences, Jansseen-Cilag, Novartis, IONIS, Medimmune, Abivax. A.B. is also a co-founder of LION TCR pte. ltd., a biotech company developing T cell receptors for treatment of virus-related cancers and chronic viral diseases. W.S.M. has acted as a consultant for Gilead; Arbutus.
Figures

References
-
- Prati D., Taioli E., Zanella A., Della Torre E., Butelli S., Del Vecchio E., Vianello L., Zanuso F., Mozzi F., Milani S., et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann. Intern. Med. 2002;137:1–10. doi: 10.7326/0003-4819-137-1-200207020-00006. - DOI - PubMed
-
- Sokal E.M., Paganelli M., Wirth S., Socha P., Vajro P., Lacaille F., Kelly D., Mieli-Vergani G. Management of chronic hepatitis B in childhood: Espghan clinical practice guidelines: Consensus of an expert panel on behalf of the european society of pediatric gastroenterology, hepatology and nutrition. J. Hepatol. 2013;59:814–829. doi: 10.1016/j.jhep.2013.05.016. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
