

Heparin and Heparin-Derivatives in Post-Subarachnoid Hemorrhage Brain Injury: A Multimodal Therapy for a Multimodal Disease
- PMID: 28468328
- PMCID: PMC6154575
- DOI: 10.3390/molecules22050724
Heparin and Heparin-Derivatives in Post-Subarachnoid Hemorrhage Brain Injury: A Multimodal Therapy for a Multimodal Disease
Abstract
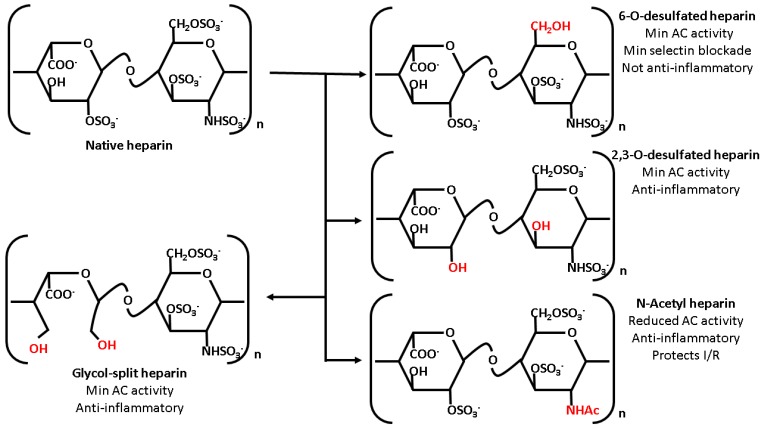
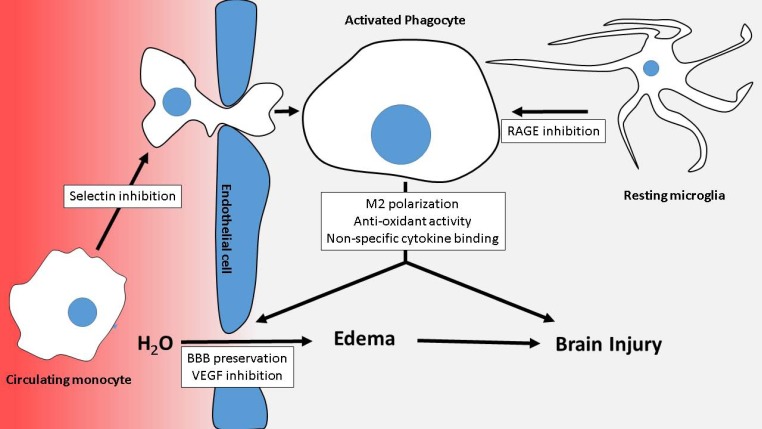
Pharmacologic efforts to improve outcomes following aneurysmal subarachnoid hemorrhage (aSAH) remain disappointing, likely owing to the complex nature of post-hemorrhage brain injury. Previous work suggests that heparin, due to the multimodal nature of its actions, reduces the incidence of clinical vasospasm and delayed cerebral ischemia that accompany the disease. This narrative review examines how heparin may mitigate the non-vasospastic pathological aspects of aSAH, particularly those related to neuroinflammation. Following a brief review of early brain injury in aSAH and heparin's general pharmacology, we discuss potential mechanistic roles of heparin therapy in treating post-aSAH inflammatory injury. These roles include reducing ischemia-reperfusion injury, preventing leukocyte extravasation, modulating phagocyte activation, countering oxidative stress, and correcting blood-brain barrier dysfunction. Following a discussion of evidence to support these mechanistic roles, we provide a brief discussion of potential complications of heparin usage in aSAH. Our review suggests that heparin's use in aSAH is not only safe, but effectively addresses a number of pathologies initiated by aSAH.
Keywords: brain injury; edema; enoxaparin; heparin; inflammation; subarachnoid hemorrhage.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Ogden J.A., Utley T., Mee E.W. Neurological and psychosocial outcome 4 to 7 years after subarachnoid hemorrhage. Neurosurgery. 1997;41:25–34. - PubMed
-
- Hackett M.L., Anderson C.S. Health outcomes 1 year after subarachnoid hemorrhage: An international population-based study. The australian cooperative research on subarachnoid hemorrhage study group. Neurology. 2000;55:658–662. - PubMed
-
- Kreiter K.T., Copeland D., Bernardini G.L., Bates J.E., Peery S., Claassen J., Du Y.E., Stern Y., Connolly E.S., Mayer S.A. Predictors of cognitive dysfunction after subarachnoid hemorrhage. Stroke. 2002;33:200–208. - PubMed
-
- Al-Khindi T., Macdonald R.L., Schweizer T.A. Cognitive and functional outcome after aneurysmal subarachnoid hemorrhage. Stroke. 2010;41:e519–e536. - PubMed
-
- Haley E.C., Jr. Measuring cognitive outcome after subarachnoid hemorrhage. Ann. Neurol. 2006;60:502–504. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
