

Universal test, treat, and keep: improving ART retention is key in cost-effective HIV control in Uganda
- PMID: 28468605
- PMCID: PMC5415795
- DOI: 10.1186/s12879-017-2420-y
Universal test, treat, and keep: improving ART retention is key in cost-effective HIV control in Uganda
Abstract
Background: With ambitious new UNAIDS targets to end AIDS by 2030, and new WHO treatment guidelines, there is increased interest in the best way to scale-up ART coverage. We investigate the cost-effectiveness of various ART scale-up options in Uganda.
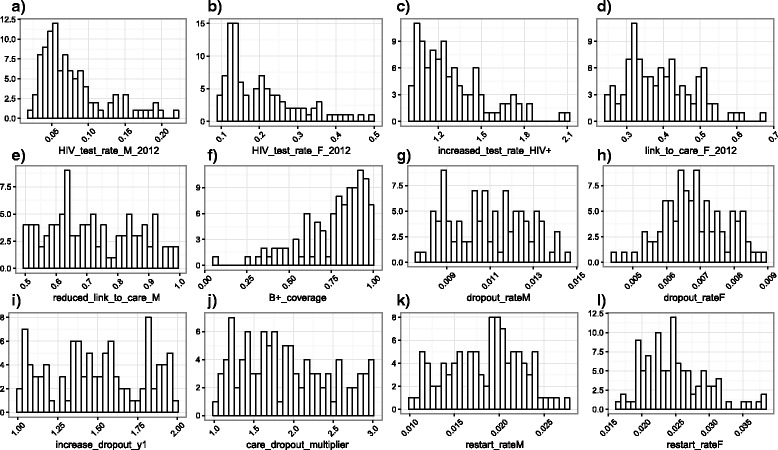
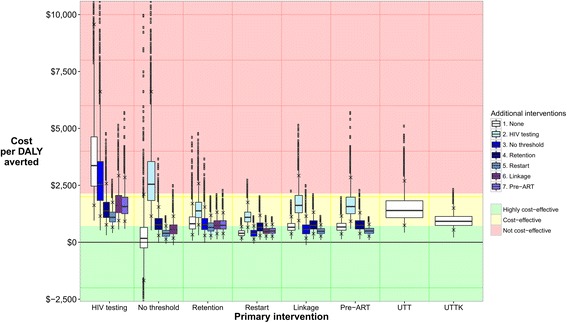
Methods: Individual-based HIV/ART model of Uganda, calibrated using history matching. 22 ART scale-up strategies were simulated from 2016 to 2030, comprising different combinations of six single interventions (1. increased HIV testing rates, 2. no CD4 threshold for ART initiation, 3. improved ART retention, 4. increased ART restart rates, 5. improved linkage to care, 6. improved pre-ART care). The incremental net monetary benefit (NMB) of each intervention was calculated, for a wide range of different willingness/ability to pay (WTP) per DALY averted (health-service perspective, 3% discount rate).
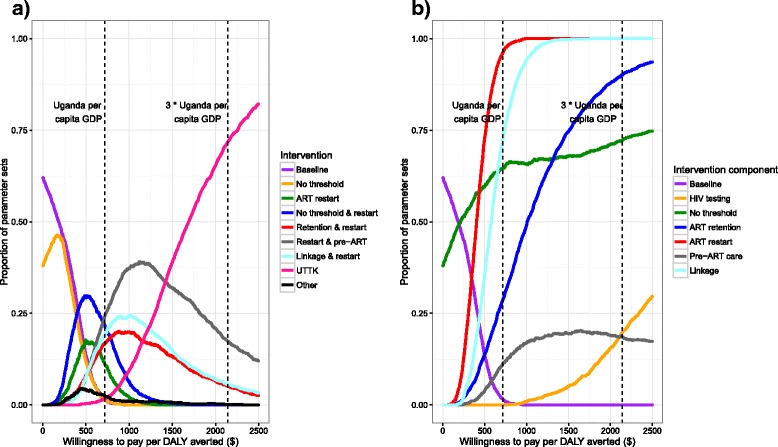
Results: For all WTP thresholds above $210, interventions including removing the CD4 threshold were likely to be most cost-effective. At a WTP of $715 (1 × per-capita-GDP) interventions to improve linkage to and retention/re-enrolment in HIV care were highly likely to be more cost-effective than interventions to increase rates of HIV testing. At higher WTP (> ~ $1690), the most cost-effective option was 'Universal Test, Treat, and Keep' (UTTK), which combines interventions 1-5 detailed above.
Conclusions: Our results support new WHO guidelines to remove the CD4 threshold for ART initiation in Uganda. With additional resources, this could be supplemented with interventions aimed at improving linkage to and/or retention in HIV care. To achieve the greatest reductions in HIV incidence, a UTTK policy should be implemented.
Keywords: ART; Cost-effectiveness; HIV; Mathematical modelling; Uganda; Universal test and treat.
Figures



References
-
- Joint United Nations Programme on HIV/AIDS: The gap report. Geneva: UNAIDS 2014.
-
- Uganda AIDS Commission: HIV and AIDS Uganda Country progress report; 2014. Kampala: Uganda AIDS Commission 2015.
-
- Joint United Nations Programme on HIV/AIDS: 90–90-90: an ambitious treatment target to help end the AIDS epidemic. Geneva: UNAIDS 2014.
-
- Uganda AIDS. Commission: national HIV AND AIDS Strategic Plan 2015/2016-2019/2020. In Uganda. 2015;
-
- Ying R, Sharma M, Celum C, Baeten JM, van Rooyen H, Hughes JP, Garnett G, Barnabas RV. Home testing and counselling to reduce HIV incidence in a generalised epidemic setting: a mathematical modelling analysis. The Lancet HIV. 2016;3(6):e275–e282. doi: 10.1016/S2352-3018(16)30009-1. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
