

Myocardial and haemodynamic responses to two fluid regimens in African children with severe malnutrition and hypovolaemic shock (AFRIM study)
- PMID: 28468633
- PMCID: PMC5415747
- DOI: 10.1186/s13054-017-1679-0
Myocardial and haemodynamic responses to two fluid regimens in African children with severe malnutrition and hypovolaemic shock (AFRIM study)
Abstract
Background: Fluid therapy in severely malnourished children is hypothesized to be deleterious owing to compromised cardiac function. We evaluated World Health Organization (WHO) fluid resuscitation guidelines for hypovolaemic shock using myocardial and haemodynamic function and safety endpoints.
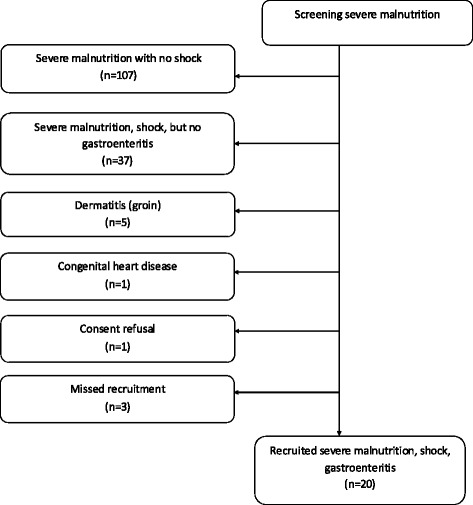
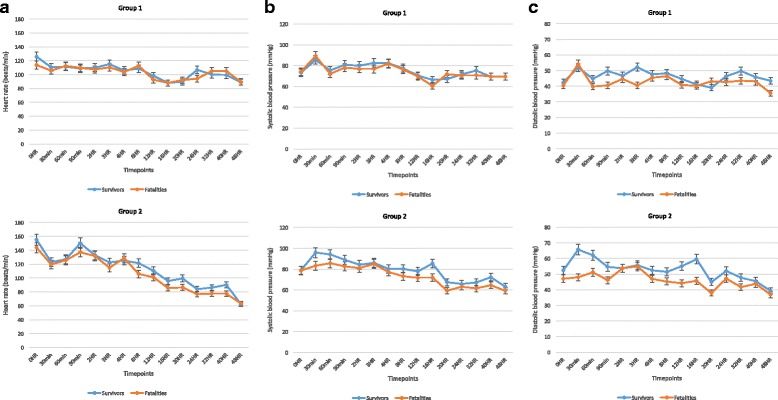
Methods: A prospective observational study of two sequential fluid management strategies was conducted at two East African hospitals. Eligible participants were severely malnourished children, aged 6-60 months, with hypovolaemic shock secondary to gastroenteritis. Group 1 received up to two boluses of 15 ml/kg/h of Ringer's lactate (RL) prior to rehydration as per WHO guidelines. Group 2 received rehydration only (10 ml/kg/h of RL) up to a maximum of 5 h. Comprehensive clinical, haemodynamic and echocardiographic data were collected from admission to day 28.
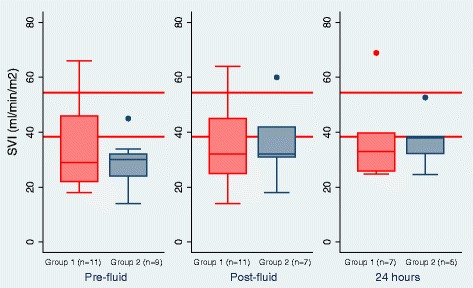
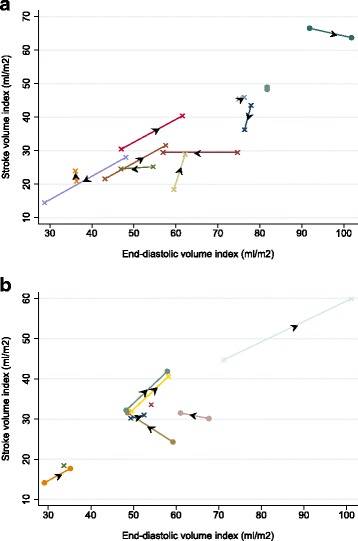
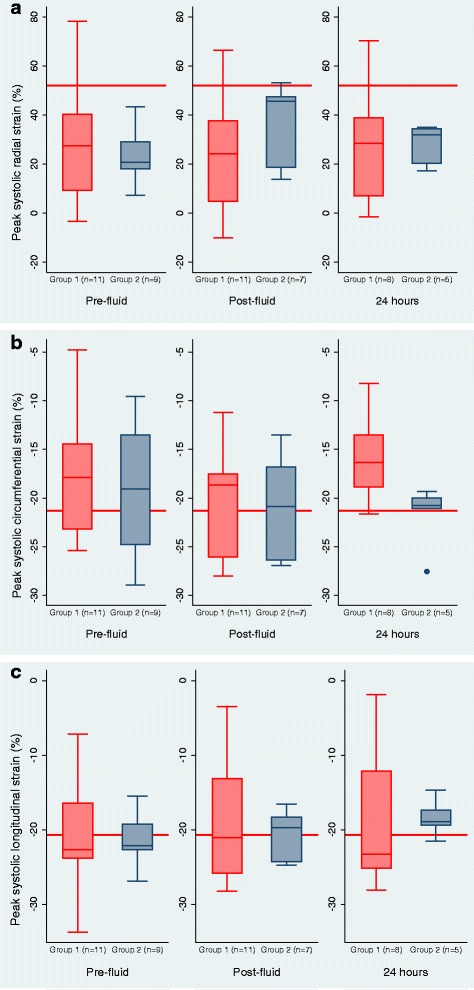
Results: Twenty children were enrolled (11 in group 1 and 9 in group 2), including 15 children (75%) with kwashiorkor, 8 (40%) with elevated brain natriuretic peptide >300 pg/ml, and 9 (45%) with markedly elevated median systemic vascular resistance index (SVRI) >1600 dscm-5/m2 indicative of severe hypovolaemia. Echocardiographic evidence of fluid-responsiveness (FR) was heterogeneous in group 1, with both increased and decreased stroke volume and myocardial fractional shortening. In group 2, these variables were more homogenous and typical of FR. Median SVRI marginally decreased post fluid administration (both groups) but remained high at 24 h. Mortality at 48 h and to day 28, respectively, was 36% (4 deaths) and 81.8% (9 deaths) in group 1 and 44% (4 deaths) and 55.6% (5 deaths) in group 2. We observed no pulmonary oedema or congestive cardiac failure on or during admission; most deaths were unrelated to fluid interventions or echocardiographic findings of response to fluids.
Conclusion: Baseline and cardiac response to fluid resuscitation do not indicate an effect of compromised cardiac function on response to fluid loading or that fluid overload is common in severely malnourished children with hypovolaemic shock. Endocrine response to shock and persistently high SVRI post fluid-therapy resuscitation may indicate a need for further research investigating enhanced fluid volumes to adequately correct volume deficit. The adverse outcomes are concerning, but appear to be unrelated to immediate fluid management.
Keywords: African; Children; Echocardiography; Fluid resuscitation; Gastroenteritis; Hypovolaemic shock; Mortality; Myocardial function; Ringers lactate; Severe malnutrition.
Figures
Comment in
-
Understanding fluid administration approaches in children with co-morbidities and septic shock.Crit Care. 2017 Aug 2;21(1):204. doi: 10.1186/s13054-017-1741-y. Crit Care. 2017. PMID: 28774323 Free PMC article. No abstract available.
-
Variability of response to the fluid bolus is again demonstrated.Crit Care. 2017 Aug 25;21(1):224. doi: 10.1186/s13054-017-1793-z. Crit Care. 2017. PMID: 28841889 Free PMC article. No abstract available.
Similar articles
-
Phase II trial of isotonic fluid resuscitation in Kenyan children with severe malnutrition and hypovolaemia.BMC Pediatr. 2010 Oct 6;10:71. doi: 10.1186/1471-2431-10-71. BMC Pediatr. 2010. PMID: 20923577 Free PMC article. Clinical Trial.
-
Fluid management of shock in severe malnutrition: what is the evidence for current guidelines and what lessons have been learned from clinical studies and trials in other pediatric populations?Food Nutr Bull. 2014 Jun;35(2 Suppl):S71-8. doi: 10.1177/15648265140352S111. Food Nutr Bull. 2014. PMID: 25069297 Free PMC article. Review.
-
A Clinical and Physiological Prospective Observational Study on the Management of Pediatric Shock in the Post-Fluid Expansion as Supportive Therapy Trial Era.Pediatr Crit Care Med. 2022 Jul 1;23(7):502-513. doi: 10.1097/PCC.0000000000002968. Epub 2022 Apr 21. Pediatr Crit Care Med. 2022. PMID: 35446796 Free PMC article.
-
Gastroenteritis aggressive versus slow treatment for rehydration (GASTRO): a phase II rehydration trial for severe dehydration: WHO plan C versus slow rehydration.BMC Med. 2019 Jul 1;17(1):122. doi: 10.1186/s12916-019-1356-z. BMC Med. 2019. PMID: 31256761 Free PMC article. Clinical Trial.
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
Cited by
-
Effectiveness of the WHO Protocol for the Management of Shock in Children With Severe Acute Malnutrition.Cureus. 2023 Sep 30;15(9):e46252. doi: 10.7759/cureus.46252. eCollection 2023 Sep. Cureus. 2023. PMID: 37908954 Free PMC article.
-
Refeeding Syndrome Developed in a Patient With Kwashiorkor Can Mimic Findings of Mitochondrial Disorder.Clin Med Insights Case Rep. 2022 Apr 30;15:11795476221093287. doi: 10.1177/11795476221093287. eCollection 2022. Clin Med Insights Case Rep. 2022. PMID: 35519509 Free PMC article.
-
The diagnosis and management of dehydration in children with wasting or nutritional edema: A systematic review.PLOS Glob Public Health. 2023 Nov 3;3(11):e0002520. doi: 10.1371/journal.pgph.0002520. eCollection 2023. PLOS Glob Public Health. 2023. PMID: 37922322 Free PMC article.
-
Variability of response to the fluid bolus is again demonstrated.Crit Care. 2017 Aug 25;21(1):224. doi: 10.1186/s13054-017-1793-z. Crit Care. 2017. PMID: 28841889 Free PMC article. No abstract available.
-
Intravenous Rehydration for Severe Acute Malnutrition with Gastroenteritis.N Engl J Med. 2025 Jun 13:10.1056/NEJMoa2505752. doi: 10.1056/NEJMoa2505752. Online ahead of print. N Engl J Med. 2025. PMID: 40513026 Free PMC article.
References
-
- WHO. Pocket book of hospital care for children 2nd edition. Guidelines for the management of common childhood illnesses. Geneva: WHO; 2013. - PubMed
-
- Alam NH, Islam S, Sattar S, Monira S, Desjeux JF. Safety of rapid intravenous rehydration and comparative efficacy of 3 oral rehydration solutions in the treatment of severely malnourished children with dehydrating cholera. J Pediatr Gastroenterol Nutr. 2009;48(3):318–27. doi: 10.1097/MPG.0b013e318180af27. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
