

CTLA4-Ig in combination with FTY720 promotes allograft survival in sensitized recipients
- PMID: 28469082
- PMCID: PMC5414557
- DOI: 10.1172/jci.insight.92033
CTLA4-Ig in combination with FTY720 promotes allograft survival in sensitized recipients
Abstract
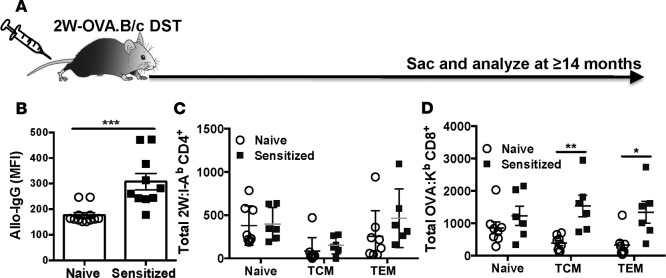
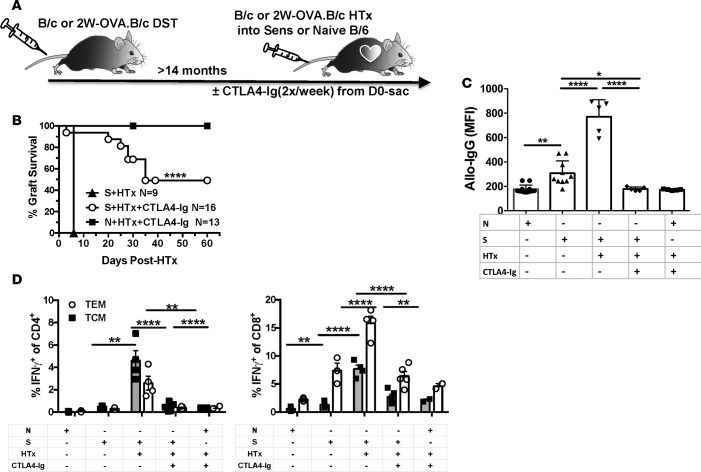
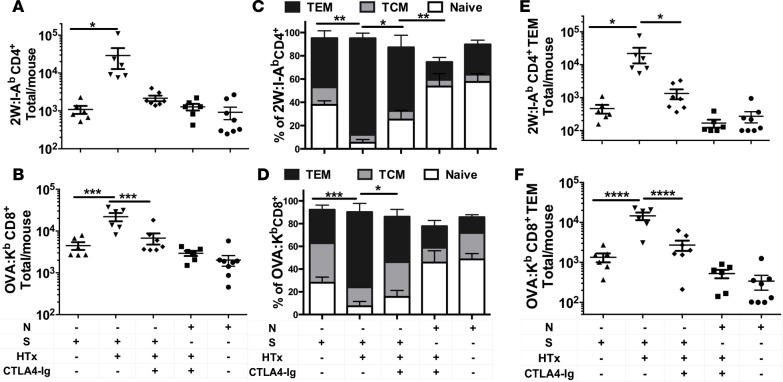
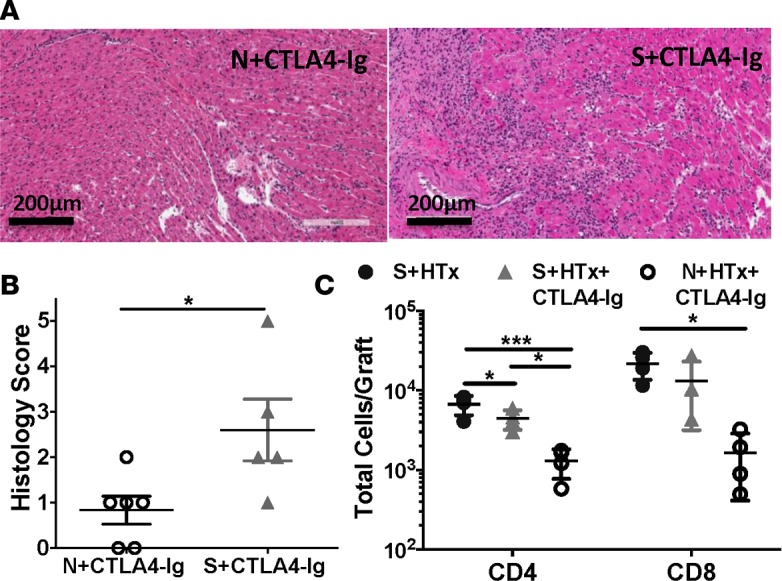
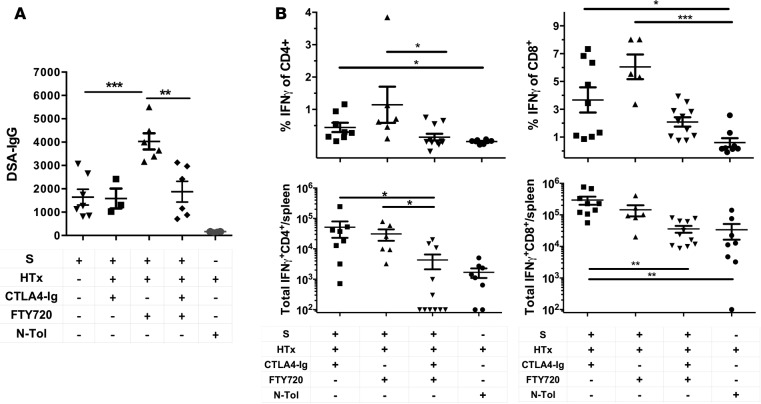
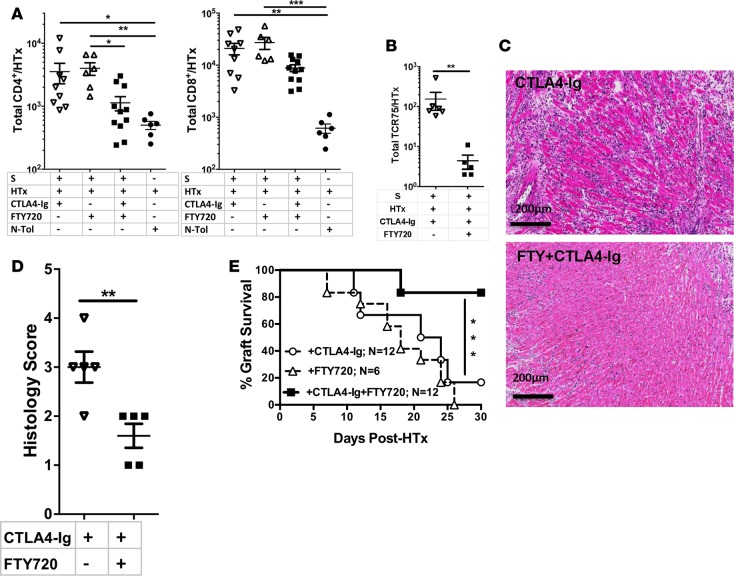
Despite recent evidence of improved graft outcomes and safety, the high incidence of early acute cellular rejection with belatacept, a high-affinity CTLA4-Ig, has limited its use in clinical transplantation. Here we define how the incomplete control of endogenous donor-reactive memory T cells results in belatacept-resistant rejection in an experimental model of BALB/c.2W-OVA donor heart transplantation into C57BL/6 recipients presensitized to donor splenocytes. These sensitized mice harbored modestly elevated numbers of endogenous donor-specific memory T cells and alloantibodies compared with naive recipients. Continuous CTLA4-Ig treatment was unexpectedly efficacious at inhibiting endogenous graft-reactive T cell expansion but was unable to inhibit late CD4+ and CD8+ T cell infiltration into the allografts, and rejection was observed in 50% of recipients by day 35 after transplantation. When CTLA4-Ig was combined with the sphingosine 1-phosphate receptor-1 (S1PR1) functional antagonist FTY720, alloantibody production was inhibited and donor-specific IFN-γ-producing T cells were reduced to levels approaching nonsensitized tolerant recipients. Late T cell recruitment into the graft was also restrained, and graft survival improved with this combination therapy. These observations suggest that a rational strategy consisting of inhibiting memory T cell expansion and trafficking into the allograft with CTLA4-Ig and FTY720 can promote allograft survival in allosensitized recipients.
Keywords: Immunology; Transplantation.
Conflict of interest statement
Figures
References
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
