

Models of Lung Transplant Research: a consensus statement from the National Heart, Lung, and Blood Institute workshop
- PMID: 28469087
- PMCID: PMC5414568
- DOI: 10.1172/jci.insight.93121
Models of Lung Transplant Research: a consensus statement from the National Heart, Lung, and Blood Institute workshop
Abstract
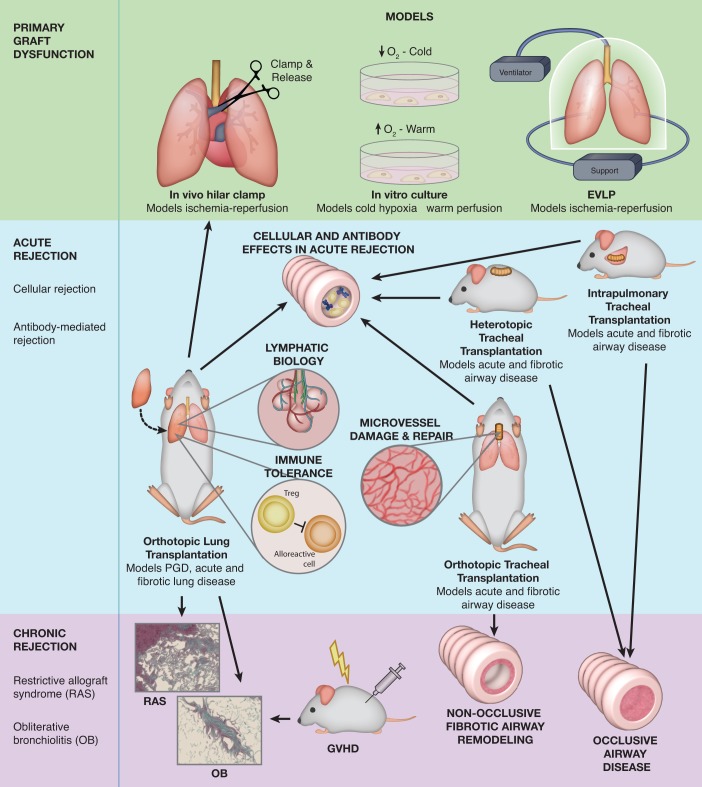
Lung transplantation, a cure for a number of end-stage lung diseases, continues to have the worst long-term outcomes when compared with other solid organ transplants. Preclinical modeling of the most common and serious lung transplantation complications are essential to better understand and mitigate the pathophysiological processes that lead to these complications. Various animal and in vitro models of lung transplant complications now exist and each of these models has unique strengths. However, significant issues, such as the required technical expertise as well as the robustness and clinical usefulness of these models, remain to be overcome or clarified. The National Heart, Lung, and Blood Institute (NHLBI) convened a workshop in March 2016 to review the state of preclinical science addressing the three most important complications of lung transplantation: primary graft dysfunction (PGD), acute rejection (AR), and chronic lung allograft dysfunction (CLAD). In addition, the participants of the workshop were tasked to make consensus recommendations on the best use of these complimentary models to close our knowledge gaps in PGD, AR, and CLAD. Their reviews and recommendations are summarized in this report. Furthermore, the participants outlined opportunities to collaborate and directions to accelerate research using these preclinical models.
Keywords: Immunology; Transplantation.
Conflict of interest statement
Figures
References
-
- Sharma AK, Fernandez LG, Awad AS, Kron IL, Laubach VE. Proinflammatory response of alveolar epithelial cells is enhanced by alveolar macrophage-produced TNF-alpha during pulmonary ischemia-reperfusion injury. Am J Physiol Lung Cell Mol Physiol. 2007;293(1):L105–L113. doi: 10.1152/ajplung.00470.2006. - DOI - PubMed
-
- Cardella JA, et al. A novel cell culture model for studying ischemia-reperfusion injury in lung transplantation. J Appl Physiol. 2000;89(4):1553–1560. - PubMed
Publication types
Grants and funding
- R01 HL095686/HL/NHLBI NIH HHS/United States
- R01 HL119218/HL/NHLBI NIH HHS/United States
- R01 HL130324/HL/NHLBI NIH HHS/United States
- R01 HL109310/HL/NHLBI NIH HHS/United States
- R01 HL133293/HL/NHLBI NIH HHS/United States
- R01 HL130275/HL/NHLBI NIH HHS/United States
- R01 HL130053/HL/NHLBI NIH HHS/United States
- R01 HL094622/HL/NHLBI NIH HHS/United States
- R01 HL092514/HL/NHLBI NIH HHS/United States
- R01 HL118017/HL/NHLBI NIH HHS/United States
- P01 HL108797/HL/NHLBI NIH HHS/United States
- R01 HL094601/HL/NHLBI NIH HHS/United States
- P30 DK054759/DK/NIDDK NIH HHS/United States
- R01 HL112990/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
