

Serum anion gap at admission as a predictor of mortality in the pediatric intensive care unit
- PMID: 28469150
- PMCID: PMC5431089
- DOI: 10.1038/s41598-017-01681-9
Serum anion gap at admission as a predictor of mortality in the pediatric intensive care unit
Abstract
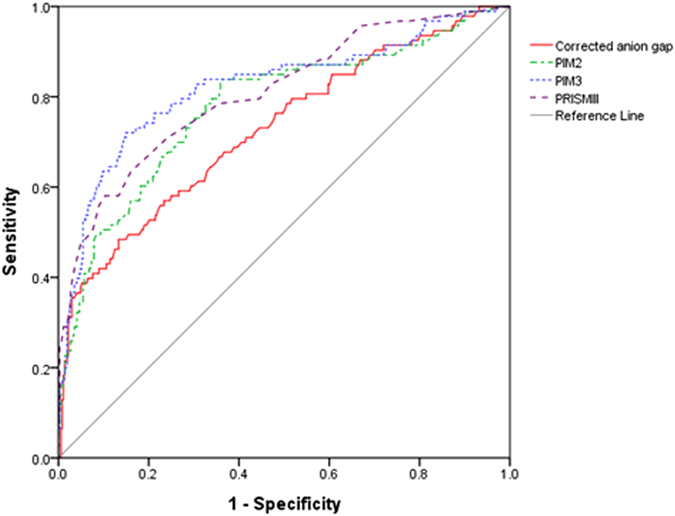
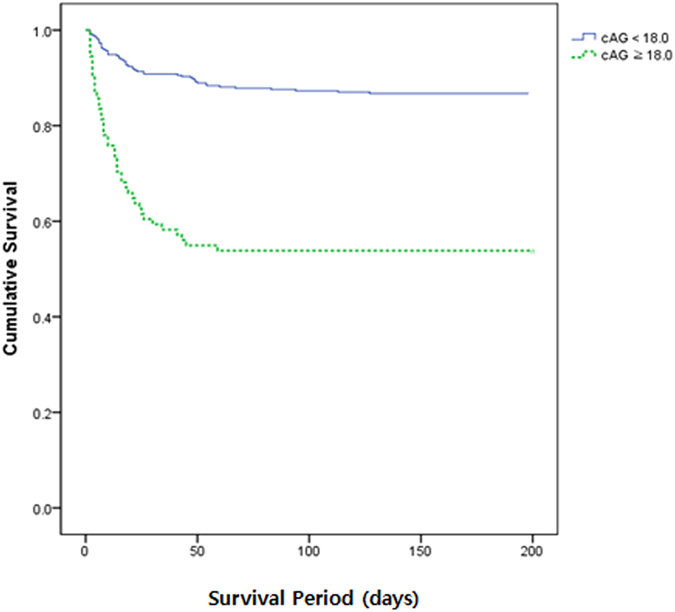
An accurate method to predict the mortality in the intensive care unit (ICU) patients has been required, especially in children. The aim of this study is to evaluate the value of serum anion gap (AG) for predicting mortality in pediatric ICU (PICU). We reviewed a data of 461 pediatric patients were collected on PICU admission. Corrected anion gap (cAG), the AG compensated for abnormal albumin levels, was significantly lower in survivors compared with nonsurvivors (p < 0.001). Multivariable logistic regression analysis identified the following variables as independent predictors of mortality; cAG (OR 1.110, 95% CI 1.06-1.17; p < 0.001), PIM3 [OR 7.583, 95% CI 1.81-31.78; p = 0.006], and PRISM III [OR 1.076, 95% CI 1.02-1.14; p = 0.008]. Comparing AUCs for mortality prediction, there were no statistically significant differences between cAG and other mortality prediction models; cAG 0.728, PIM2 0.779, PIM3 0.822, and PRISM III 0.808. The corporation of cAG to pre-existing mortality prediction models was significantly more accurate at predicting mortality than using any of these models alone. We concluded that cAG at ICU admission may be used to predict mortality in children, regardless of underlying etiology. And the incorporation of cAG to pre-existing mortality prediction models might improve predictability.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
Similar articles
-
Association between anion gap and mortality of aortic aneurysm in intensive care unit after open surgery.BMC Cardiovasc Disord. 2021 Sep 23;21(1):458. doi: 10.1186/s12872-021-02263-4. BMC Cardiovasc Disord. 2021. PMID: 34556051 Free PMC article.
-
Metabolic acidosis in patients with severe sepsis and septic shock: a longitudinal quantitative study.Crit Care Med. 2009 Oct;37(10):2733-9. doi: 10.1097/ccm.0b013e3181a59165. Crit Care Med. 2009. PMID: 19885998
-
Diagnosis of acid-base derangements and mortality prediction in the trauma intensive care unit: the physiochemical approach.J Trauma. 2005 Feb;58(2):238-43. doi: 10.1097/01.ta.0000152535.97968.4e. J Trauma. 2005. PMID: 15706182
-
Prognostic value of anion gap for patients with heart failure: a systematic review and meta-analysis.BMC Cardiovasc Disord. 2024 Dec 20;24(1):727. doi: 10.1186/s12872-024-04420-x. BMC Cardiovasc Disord. 2024. PMID: 39707227 Free PMC article.
-
The serum anion gap in the evaluation of acid-base disorders: what are its limitations and can its effectiveness be improved?Clin J Am Soc Nephrol. 2013 Nov;8(11):2018-24. doi: 10.2215/CJN.04040413. Epub 2013 Jul 5. Clin J Am Soc Nephrol. 2013. PMID: 23833313 Free PMC article. Review.
Cited by
-
Association between anion gap and mortality of aortic aneurysm in intensive care unit after open surgery.BMC Cardiovasc Disord. 2021 Sep 23;21(1):458. doi: 10.1186/s12872-021-02263-4. BMC Cardiovasc Disord. 2021. PMID: 34556051 Free PMC article.
-
Normal Anion Gap Metabolic Acidosis in Pediatric Acute Diarrhea: A Menace or an Innocent Bystander?Indian J Crit Care Med. 2022 Dec;26(12):1235-1236. doi: 10.5005/jp-journals-10071-24371. Indian J Crit Care Med. 2022. PMID: 36755625 Free PMC article.
-
A New Insight Into Missing Data in Intensive Care Unit Patient Profiles: Observational Study.JMIR Med Inform. 2019 Jan 8;7(1):e11605. doi: 10.2196/11605. JMIR Med Inform. 2019. PMID: 30622091 Free PMC article.
-
Association between anion gap/calcium ratio and 30-day all-cause mortality in sepsis patients with diabetes mellitus.Sci Rep. 2024 Dec 28;14(1):31275. doi: 10.1038/s41598-024-82700-4. Sci Rep. 2024. PMID: 39732874 Free PMC article.
-
Development of a model for predicting mortality of breast cancer admitted to Intensive Care Unit.Afr Health Sci. 2022 Sep;22(3):155-165. doi: 10.4314/ahs.v22i3.18. Afr Health Sci. 2022. PMID: 36910387 Free PMC article.
References
-
- Imran MN, et al. Early predictors of mortality in pneumococcal bacteraemia. Ann Acad Med Singap. 2005;34:426–431. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Miscellaneous
