

Compromised neuroplasticity in cigarette smokers under nicotine withdrawal is restituted by the nicotinic α4β2-receptor partial agonist varenicline
- PMID: 28469204
- PMCID: PMC5431184
- DOI: 10.1038/s41598-017-01428-6
Compromised neuroplasticity in cigarette smokers under nicotine withdrawal is restituted by the nicotinic α4β2-receptor partial agonist varenicline
Abstract
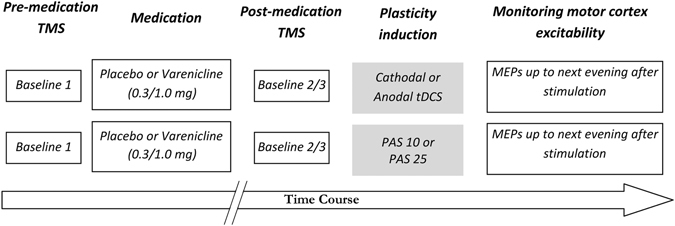
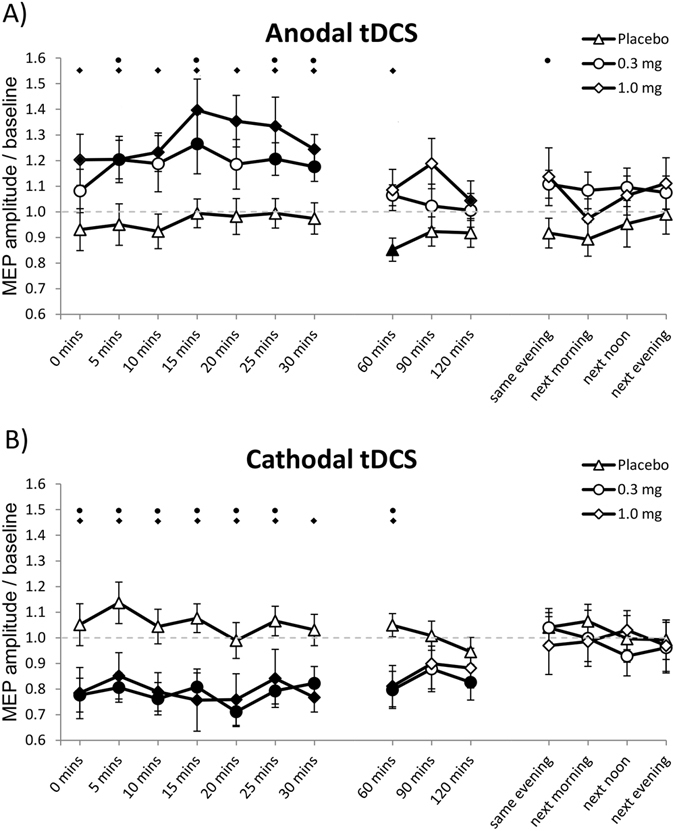
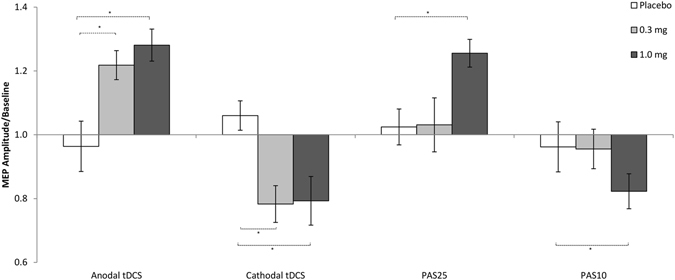
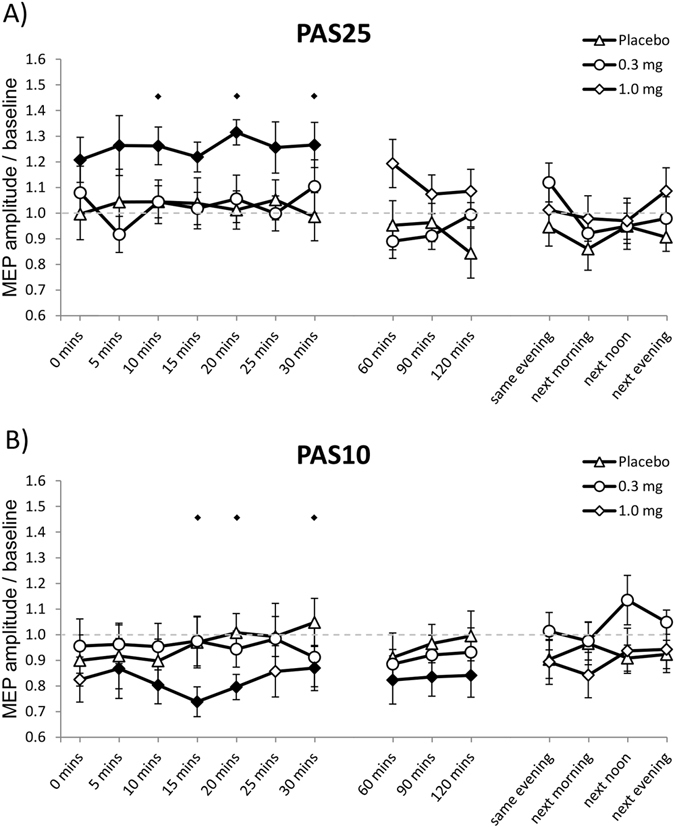
Nicotine modulates neuroplasticity and improves cognitive functions in animals and humans. In the brain of smoking individuals, calcium-dependent plasticity induced by non-invasive brain stimulation methods such as transcranial direct current stimulation (tDCS) and paired associative stimulation (PAS) is impaired by nicotine withdrawal, but partially re-established after nicotine re-administration. In order to investigate the underlying mechanism further, we tested the impact of the α4β2-nicotinic receptor partial agonist varenicline on focal and non-focal plasticity in smokers during nicotine withdrawal, induced by PAS and tDCS, respectively. We administered low (0.3 mg) and high (1.0 mg) single doses of varenicline or placebo medication before stimulation over the left motor cortex of 20 healthy smokers under nicotine withdrawal. Motor cortex excitability was monitored by single-pulse transcranial magnetic stimulation-induced motor evoked potential amplitudes for 36 hours after plasticity induction. Stimulation-induced plasticity was absent under placebo medication, whereas it was present in all conditions under high dose. Low dose restituted only tDCS-induced non-focal plasticity, producing no significant impact on focal plasticity. High dose varenicline also prolonged inhibitory plasticity. These results are comparable to the impact of nicotine on withdrawal-related impaired plasticity in smokers and suggest that α4β2 nicotinic receptors are relevantly involved in plasticity deficits and restitution in smokers.
Conflict of interest statement
M.-F. Kuo, J. Grundey and G. Batsikadze received no financial support, and no compensation has been received from any individual or corporate entity over the past 3 years for research or professional service, and there are no personal financial holdings that could be perceived as constituting a potential conflict of interest. A. Hasan has received paid speakership by Desitin and Otsuka and BAK. He was member of a Roche and a Lundbeck Advisory Board. W. Paulus is member of the Advisory Boards of EBS Technologies and Precisis AG. M.A. Nitsche is member of the Advisory Board of Neuroelectronics.
Figures
Similar articles
-
Effect of the Nicotinic α4β2-receptor Partial Agonist Varenicline on Non-invasive Brain Stimulation-Induced Neuroplasticity in the Human Motor Cortex.Cereb Cortex. 2015 Sep;25(9):3249-59. doi: 10.1093/cercor/bhu126. Epub 2014 Jun 10. Cereb Cortex. 2015. PMID: 24917274
-
Neuroplasticity in cigarette smokers is altered under withdrawal and partially restituted by nicotine exposition.J Neurosci. 2012 Mar 21;32(12):4156-62. doi: 10.1523/JNEUROSCI.3660-11.2012. J Neurosci. 2012. PMID: 22442079 Free PMC article. Clinical Trial.
-
Nicotine modulates human brain plasticity via calcium-dependent mechanisms.J Physiol. 2018 Nov;596(22):5429-5441. doi: 10.1113/JP276502. Epub 2018 Oct 17. J Physiol. 2018. PMID: 30218585 Free PMC article.
-
The neurobiological basis for partial agonist treatment of nicotine dependence: varenicline.Int J Clin Pract. 2006 May;60(5):571-6. doi: 10.1111/j.1368-5031.2006.00955.x. Int J Clin Pract. 2006. PMID: 16700857 Review.
-
Neural mechanisms underlying nicotine dependence.Addiction. 1994 Nov;89(11):1419-23. doi: 10.1111/j.1360-0443.1994.tb03738.x. Addiction. 1994. PMID: 7841851 Review.
Cited by
-
Effect of Paired Associative Stimulation on Corticomotor Excitability in Chronic Smokers.Brain Sci. 2019 Mar 15;9(3):62. doi: 10.3390/brainsci9030062. Brain Sci. 2019. PMID: 30875969 Free PMC article.
-
Active versus sham transcranial direct current stimulation (tDCS) as an adjunct to varenicline treatment for smoking cessation: Study protocol for a double-blind single dummy randomized controlled trial.PLoS One. 2022 Dec 8;17(12):e0277408. doi: 10.1371/journal.pone.0277408. eCollection 2022. PLoS One. 2022. PMID: 36480510 Free PMC article.
-
Chimera dynamics in an array of coupled FitzHugh-Nagumo system with shift of close neighbors.Heliyon. 2020 Apr 6;6(4):e03739. doi: 10.1016/j.heliyon.2020.e03739. eCollection 2020 Apr. Heliyon. 2020. PMID: 32280805 Free PMC article.
-
Transcranial electrical and magnetic stimulation (tES and TMS) for addiction medicine: A consensus paper on the present state of the science and the road ahead.Neurosci Biobehav Rev. 2019 Sep;104:118-140. doi: 10.1016/j.neubiorev.2019.06.007. Epub 2019 Jul 2. Neurosci Biobehav Rev. 2019. PMID: 31271802 Free PMC article.
-
Time-Varying Functional Connectivity Decreases as a Function of Acute Nicotine Abstinence.Biol Psychiatry Cogn Neurosci Neuroimaging. 2021 Apr;6(4):459-469. doi: 10.1016/j.bpsc.2020.10.004. Epub 2020 Oct 19. Biol Psychiatry Cogn Neurosci Neuroimaging. 2021. PMID: 33436331 Free PMC article.
References
-
- Sherwood N. Effects of Nicotine on Human Psychomotor Performance. Hum Psychopharm Clin. 1993;8:155–184. doi: 10.1002/hup.470080303. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
