

Hepatocyte Growth Factor/C-Met Axis in Thyroid Cancer: From Diagnostic Biomarker to Therapeutic Target
- PMID: 28469401
- PMCID: PMC5391983
- DOI: 10.1177/1177271917701126
Hepatocyte Growth Factor/C-Met Axis in Thyroid Cancer: From Diagnostic Biomarker to Therapeutic Target
Abstract
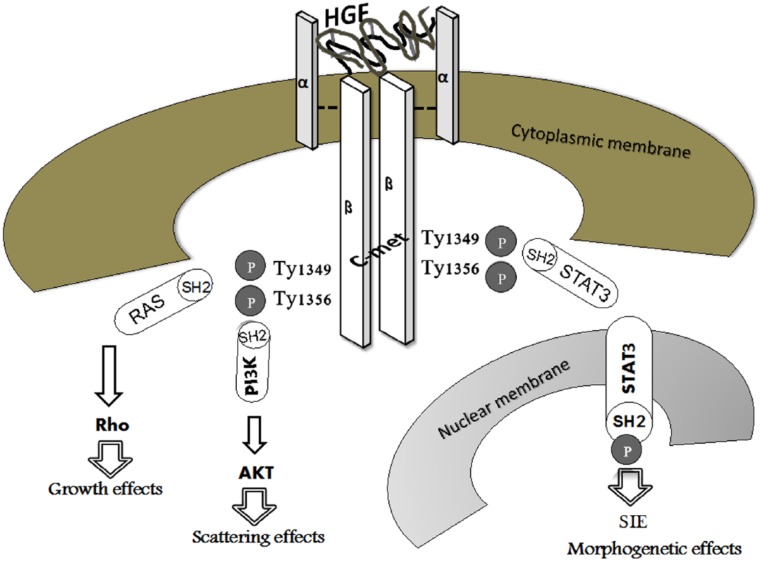
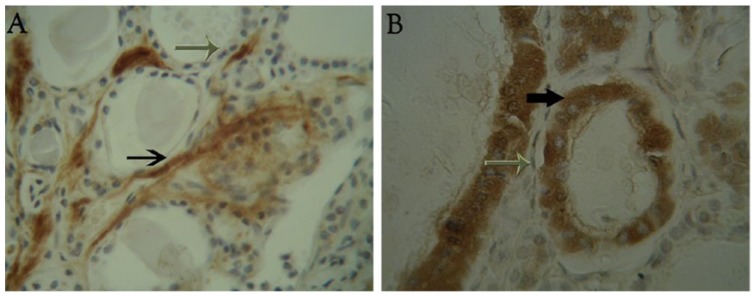
The hepatocyte growth factor (HGF)/c-met axis plays a crucial role in cancer development by promoting cellular proliferation, motility, and morphogenesis, as well as angiogenesis. Different cellular distributions of both the ligand and the receptor in benign vs malignant lesions indicate this biological system as a candidate for a diagnostic biomarker of malignancy occurring in endocrine glands, such as the thyroid and pituitary. Furthermore, the HGF/c-met expression may help to identify a subset of patients eligible for potential targeted therapies with HGF/c-met inhibitors or antagonists in thyroid tumour, as well as in other malignancies. This may be relevant for iodine-refractory cancers, the treatment of which is still a major challenge. With this in mind, HGF/c-met expression in thyroid cancer tissue may be useful for prognostic and therapeutic stratification of patients.
Keywords: HGF/c-met axis; diagnostic biomarker; therapeutic target; thyroid cancer.
Conflict of interest statement
DECLARATION OF CONFLICTING INTERESTS: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Disclosures and Ethics The authors have provided to the publisher with signed confirmation of compliance with legal and ethical obligations including, but not limited to, the following: authorship and contributorship, conflicts of interest, privacy, and confidentiality. The authors have read and confirmed their agreement with the ICMJE authorship and conflict of interest criteria. The authors have also confirmed that this article is unique and not under consideration or published in any other publication, and that they have permission from rights holders to reproduce any copyrighted material. The authors have nothing to disclose.
Figures
Similar articles
-
Role of HGF/MET axis in resistance of lung cancer to contemporary management.Transl Lung Cancer Res. 2012 Sep;1(3):179-93. doi: 10.3978/j.issn.2218-6751.2012.09.04. Transl Lung Cancer Res. 2012. PMID: 25806180 Free PMC article. Review.
-
Activation of the hepatocyte growth factor (HGF)-Met system in papillary thyroid cancer: biological effects of HGF in thyroid cancer cells depend on Met expression levels.Endocrinology. 2004 Sep;145(9):4355-65. doi: 10.1210/en.2003-1762. Epub 2004 Jun 10. Endocrinology. 2004. PMID: 15192042
-
HGF/MET pathway aberrations as diagnostic, prognostic, and predictive biomarkers in human cancers.Crit Rev Clin Lab Sci. 2019 Dec;56(8):533-566. doi: 10.1080/10408363.2019.1653821. Epub 2019 Sep 12. Crit Rev Clin Lab Sci. 2019. PMID: 31512514 Review.
-
Status of Agents Targeting the HGF/c-Met Axis in Lung Cancer.Cancers (Basel). 2018 Aug 21;10(9):280. doi: 10.3390/cancers10090280. Cancers (Basel). 2018. PMID: 30134579 Free PMC article. Review.
-
Targeting met mediated epithelial-mesenchymal transition in the treatment of breast cancer.Clin Transl Med. 2014 Dec;3(1):30. doi: 10.1186/s40169-014-0030-5. Epub 2014 Sep 26. Clin Transl Med. 2014. PMID: 26932375 Free PMC article.
Cited by
-
Multi-Omics and Management of Follicular Carcinoma of the Thyroid.Biomedicines. 2023 Apr 19;11(4):1217. doi: 10.3390/biomedicines11041217. Biomedicines. 2023. PMID: 37189835 Free PMC article. Review.
-
Update on International Medical Taxonomies of Biomarkers and Their Applications in Management of Thyroid Cancers.Diagnostics (Basel). 2022 Mar 9;12(3):662. doi: 10.3390/diagnostics12030662. Diagnostics (Basel). 2022. PMID: 35328215 Free PMC article. Review.
-
c-Met: A Promising Therapeutic Target in Bladder Cancer.Cancer Manag Res. 2022 Aug 8;14:2379-2388. doi: 10.2147/CMAR.S369175. eCollection 2022. Cancer Manag Res. 2022. PMID: 35967753 Free PMC article. Review.
-
MET overexpression and activation favors invasiveness in a model of anaplastic thyroid cancer.Oncotarget. 2019 Mar 19;10(23):2320-2334. doi: 10.18632/oncotarget.26798. eCollection 2019 Mar 19. Oncotarget. 2019. PMID: 31040922 Free PMC article.
-
Paeoniflorin Inhibits EMT and Angiogenesis in Human Glioblastoma via K63-Linked C-Met Polyubiquitination-Dependent Autophagic Degradation.Front Oncol. 2022 Jul 26;12:785345. doi: 10.3389/fonc.2022.785345. eCollection 2022. Front Oncol. 2022. PMID: 35957872 Free PMC article.
References
-
- Howlader N, Noone AM, Krapcho M, et al. eds. SEER Cancer Statistics Review, 1975–2010. Bethesda, MD: National Cancer Institute; http://seer.cancer.gov/csr/1975_2010/. Published April 2013.
-
- Aschebrook-Kilfoy B, Schechter RB, Shih YC, et al. The clinical and economic burden of a sustained increase in thyroid cancer incidence. Cancer Epidemiol Biomarkers Prev. 2013;22:1252–1259. - PubMed
-
- Albores-Saavedra J, Henson DE, Glazer E, Schwartz AM. Changing patterns in the incidence and survival of thyroid cancer with follicular phenotype – papillary, follicular, and anaplastic: a morphological and epidemiological study. Endocr Pathol. 2007;18:1–7. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
