

Hospital days attributable to immune reconstitution inflammatory syndrome in persons living with HIV before and after the 2012 DHHS HIV guidelines
- PMID: 28469696
- PMCID: PMC5414162
- DOI: 10.1186/s12981-017-0152-0
Hospital days attributable to immune reconstitution inflammatory syndrome in persons living with HIV before and after the 2012 DHHS HIV guidelines
Erratum in
-
Erratum to: Hospital days attributable to immune reconstitution inflammatory syndrome in persons living with HIV before and after the 2012 DHHS HIV guidelines.AIDS Res Ther. 2017 May 22;14:29. doi: 10.1186/s12981-017-0155-x. eCollection 2017. AIDS Res Ther. 2017. PMID: 28539969 Free PMC article.
Abstract
Background: Immune reconstitution inflammatory syndrome (IRIS) can manifest with initiation or reintroduction of antiretroviral therapy (ART) in persons living with HIV (PLWH). In 2012, updated United States treatment guidelines recommended initiation of ART for all PLWH regardless of CD4 count. The objectives of this study were to quantify hospital usage attributable to IRIS and assess the reasons for hospitalization in PLWH before and after the guideline update.
Methods: Subjects were PLWH between 18-89 years of age who were hospitalized between November 1, 2009 and July 31, 2014. Equivalent time periods before and after updated treatment guidelines were considered, and designated as Time Period 1 and Time Period 2, respectively. IRIS-attributable hospitalizations were identified by ICD9 codes and electronic medical record searches with subsequent review and confirmation. For hospitalizations that were not confirmed as being IRIS-attributable, primary discharge diagnoses were reviewed.
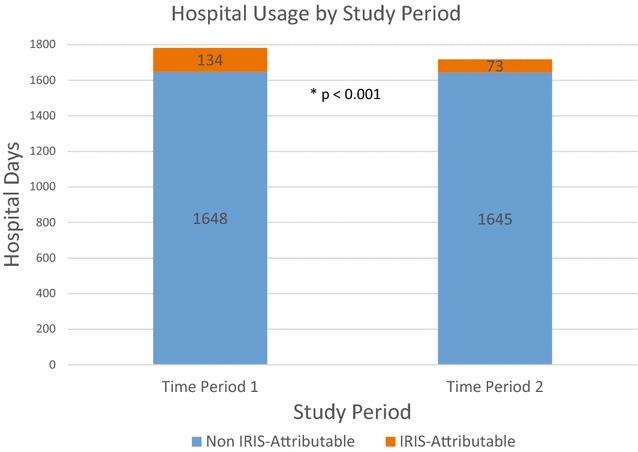
Results: A total of 278 PLWH were hospitalized 521 times throughout the study period. Time Period 1 had 9 PLWH with 12 IRIS-attributable hospitalizations while Time Period 2 had 6 PLWH with 9 IRIS-attributable hospitalizations. A larger proportion of IRIS-attributable hospital days was observed in Time Period 1 compared to Time Period 2 (7.5 vs 4.2%; p < 0.001). Median length of stay for IRIS-attributable hospitalizations was longer than for other diagnoses, particularly during Time Period 1 (12.0 vs 4.0; p = 0.05). The most common causes for hospitalizations in PLWH were non AIDS-defining infection, AIDS-defining malignancy, and gastrointestinal. PLWH who had HIV viral suppression (<200 copies/mL) accounted for 34 and 24% of hospitalizations in Time Periods 1 and 2 respectively.
Conclusions: Hospitalizations for PLWH continue at high rates and IRIS is a significant contributing factor. In our single-center study, there was a lower number of IRIS-attributable hospitalizations and IRIS-attributable hospital days in Time Period 2 compared with Time Period 1. The hospital burden of IRIS may decrease over time as more PLWH are started on ART earlier in the course of infection. This study highlights the continued importance of early diagnosis and linkage to care of those infected with HIV, so that morbidity and costs associated with IRIS continue to decline.
Keywords: AIDS; Acquired immunodeficiency syndrome; HIV; Hospitalization; Human immunodeficiency virus; IRIS; Immune reconstitution inflammatory syndrome; Practice guidelines; United States Dept. of Health and Human Services.
Figures
References
-
- Teeraananchai S, Kerr S, Ruxrungtham K. Life expectancy of HIV-positive people after starting combination antiretroviral therapy: a meta-analysis. HIV Med [Epub ahead of print]. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
