

Anxiety disorders
- PMID: 28470168
- PMCID: PMC11009418
- DOI: 10.1038/nrdp.2017.24
Anxiety disorders
Erratum in
-
Correction: Anxiety disorders.Nat Rev Dis Primers. 2017 Dec 14;3:17100. doi: 10.1038/nrdp.2017.100. Nat Rev Dis Primers. 2017. PMID: 29239346
Abstract
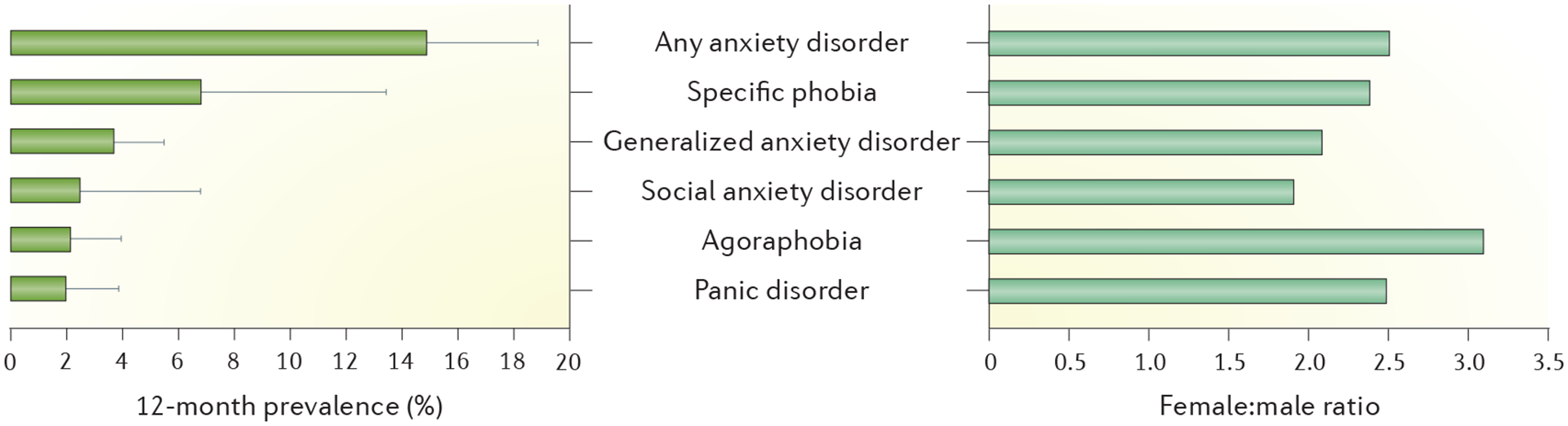
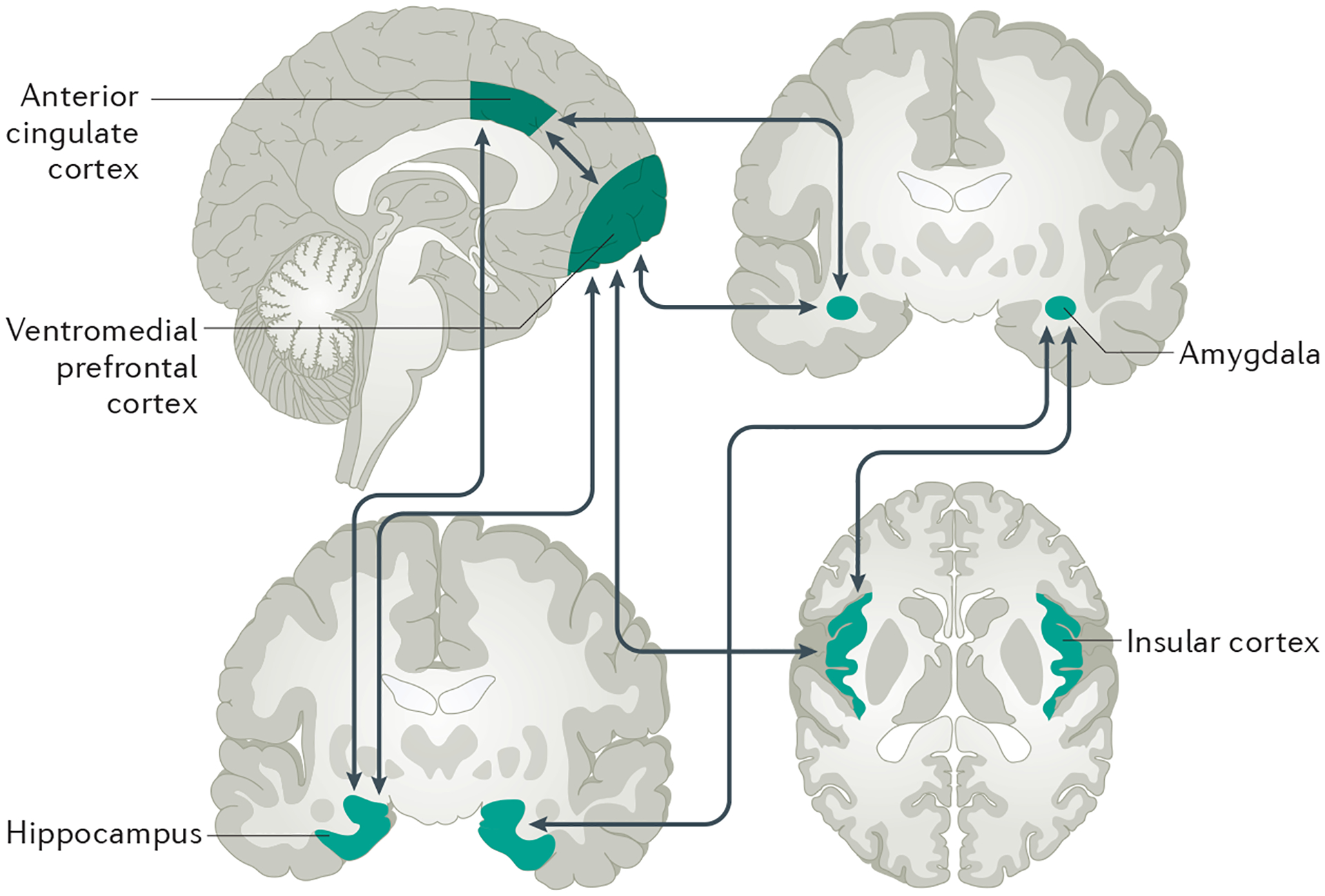
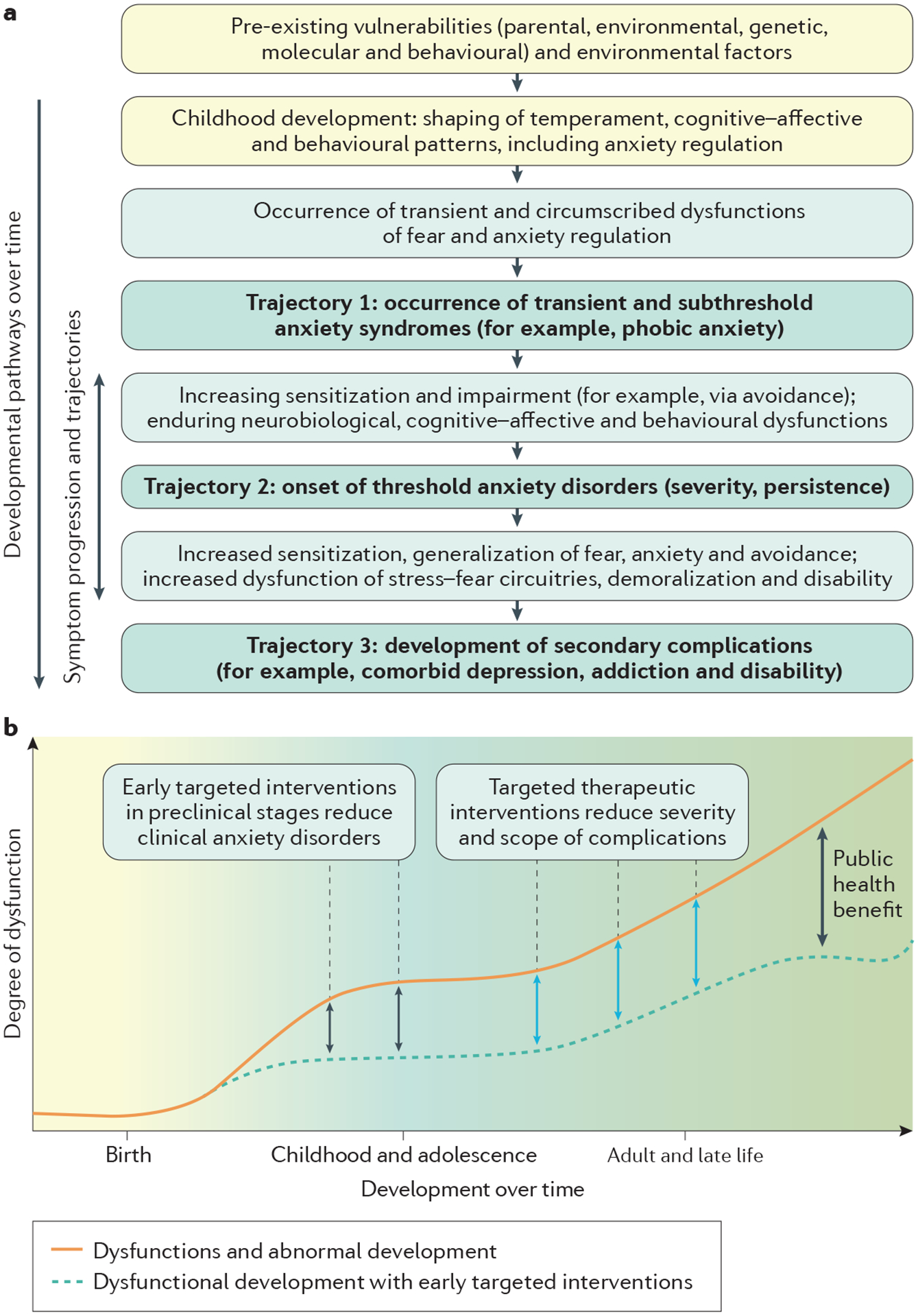
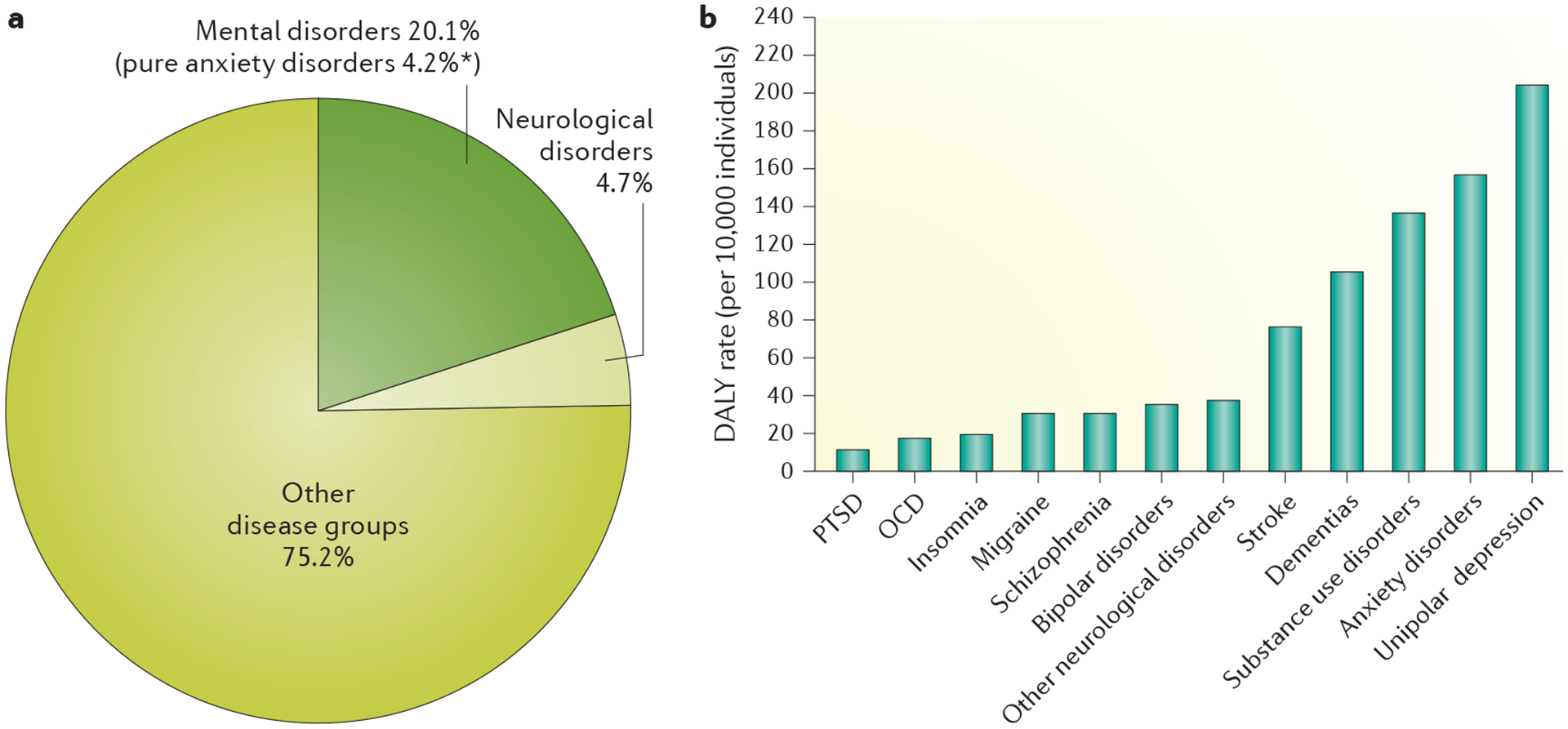
Anxiety disorders constitute the largest group of mental disorders in most western societies and are a leading cause of disability. The essential features of anxiety disorders are excessive and enduring fear, anxiety or avoidance of perceived threats, and can also include panic attacks. Although the neurobiology of individual anxiety disorders is largely unknown, some generalizations have been identified for most disorders, such as alterations in the limbic system, dysfunction of the hypothalamic-pituitary-adrenal axis and genetic factors. In addition, general risk factors for anxiety disorders include female sex and a family history of anxiety, although disorder-specific risk factors have also been identified. The diagnostic criteria for anxiety disorders varies for the individual disorders, but are generally similar across the two most common classification systems: the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) and the International Classification of Diseases, Tenth Edition (ICD-10). Despite their public health significance, the vast majority of anxiety disorders remain undetected and untreated by health care systems, even in economically advanced countries. If untreated, these disorders are usually chronic with waxing and waning symptoms. Impairments associated with anxiety disorders range from limitations in role functioning to severe disabilities, such as the patient being unable to leave their home.
Conflict of interest statement
Competing interests
M.B.S. has received consulting fees in the past 3 years from Actelion Pharmaceuticals, Janssen, Neurocrine Biosciences, and Pfizer, and stock options from Oxeia Biopharmaceuticals and Resilience Therapeutics. M.B.S. also receives editorial honoraria from the journal
Figures

References
-
- Wittchen HU et al. The size and burden of mental disorders and other disorders of the brain in Europe 2010. Eur. Neuropsychopharmacol 21, 655–679 (2D). - PubMed
-
Provides the most recent state-of-the-art summary of epidemiological evidence of anxiety disorders and their associated burden in Europe.
-
- Christopher P & Murray JL Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 388, 1659–1724 (2016). - PMC - PubMed
-
- Kessler RC, Ruscio AM, Shear K & Wittchen H-U Epidemiology of anxiety disorders. Curr. Top. Behav. Neurosci 2, 21–35 (2010). - PubMed
-
Overviews the prevalence of and risk factors for anxiety disorders.
-
- Beesdo K, Knappe S & Pine DS Anxiety and anxiety disorders in children and adolescents: developmental issues and implications for DSM-V. Psychiatr. Clin. North Am 32, 483–524 (2009). - PMC - PubMed
-
One of the few available prospective, longitudinal epidemiological studies that provides valid incidence data on anxiety disorders as well as the risk for secondary depression.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
