

Long or redundant leaflet complicating transcatheter mitral valve replacement: Case vignettes that advocate for removal or reduction of the anterior mitral leaflet
- PMID: 28471059
- PMCID: PMC5671373
- DOI: 10.1002/ccd.27054
Long or redundant leaflet complicating transcatheter mitral valve replacement: Case vignettes that advocate for removal or reduction of the anterior mitral leaflet
Abstract
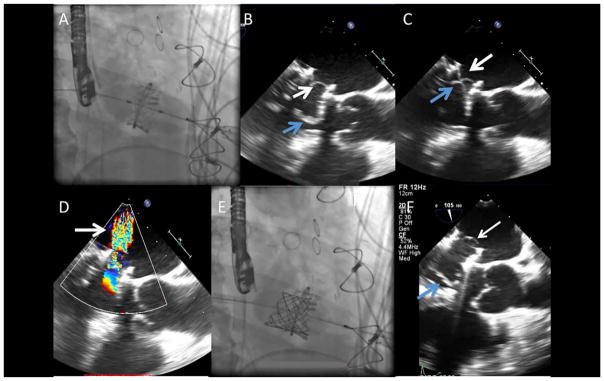
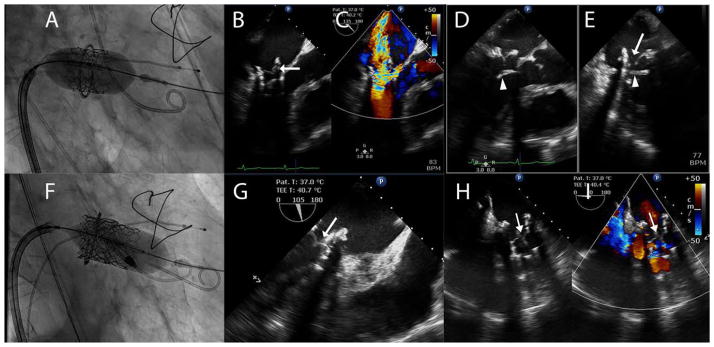
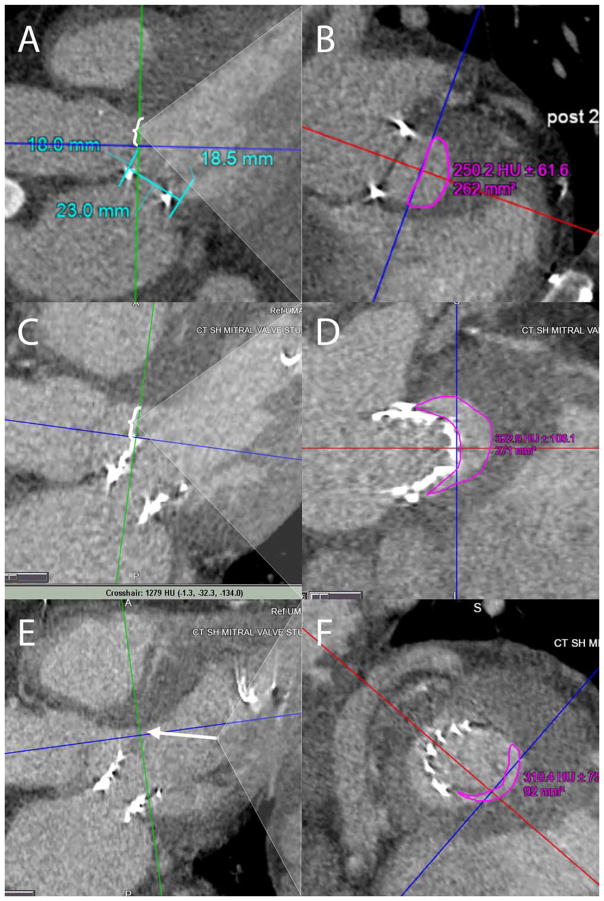
Transcatheter mitral valve replacement (TMVR) procedures can be an alternative to surgical valve replacement for high surgical risk patients with bioprosthetic mitral valves, annuloplasty rings, or severe mitral annular calcification (MAC). TMVR can trigger acute left ventricular outflow tract (LVOT) obstruction from permanent displacement of the native anterior mitral leaflet toward the left ventricular septum, more often among patients undergoing valve-in-ring and valve-in-MAC procedures. Although acute LVOT obstruction is well described in the literature, there are important additional complications of TMVR related to the length and/or redundancy of the anterior mitral valve that have been recognized after mitral valve surgery and have not been previously reported in the setting of TMVR. These additional complications include acute mitral regurgitation secondary to prolapsing native leaflet through the TMVR, frozen TMVR leaflet secondary to overhanging native leaflet and late LVOT obstruction in the neo-LVOT secondary to long native leaflet. Preprocedural planning with imaging (echocardiography and computed tomography) and measurement of anterior mitral leaflet length is critical important in understanding the risk for these complications. As transcatheter mitral valve technology proliferates, interactions with the anterior mitral leaflet after TMVR may be more frequent than initially anticipated. We believe that there is no advantage to an intact anterior leaflet and advocate removal or reduction of the leaflet prior to TMVR. © 2017 Wiley Periodicals, Inc.
Keywords: complications; redundant anterior leaflet; transcatheter mitral valve replacement; valve-in-MAC; valve-in-native; valve-in-ring; valve-in-valve.
© 2017 Wiley Periodicals, Inc.
Conflict of interest statement
Conflict of interest: Adam Greenbaum is a proctor for Edwards Lifesciences and Abiomed. Stamatios Lerakis is a consultant for Abbott Vascular. Gaetano Paone is a proctor for Edwards Lifesciences. Vinod Thourani is a consultant for Edwards Lifesciences, Maquet, St Jude Medical, and Sorin. He is also co-founder and stock holder of Apica. Vasilis Babaliaros MD, FACC is a consultant for Abbott Vascular and Edwards Lifesciences. The other authors have nothing to disclose.
Figures
References
-
- De Weger A, Ewe SH, Delgado V, Bax JJ. First-in-man implantation of a trans-catheter aortic valve in a mitral annuloplasty ring: Novel treatment modality for failed mitral valve repair. Eur J Cardiothorac Surg. 2011;39:1054–1056. - PubMed
-
- Petronio A, Giannini C, De Carlo M, Guarracino F. Antegrade percutaneous valve implantation for mitral ring dysfunction, a challenging case. Catheter Cardiovasc Interv. 2012;80:700–703. - PubMed
-
- Seiffert M, Conradi L, Baldus S, Schirmer J, Knap M, Blankenberg S, Reichenspurner H, Treede H. Transcatheter mitral valve-in-valve implantation in patients with degenerated bioprostheses. JACC Cardiovasc Interv. 2012;5:341–349. - PubMed
-
- Guerrero M, Dvir D, Himbert D, Urena M, Eleid M, Wang DD, Greenbaum A, Mahadevan VS, Holzhey D, O’Hair D, Dumonteil N, Rodés-Cabau J, Piazza N, Palma JH, DeLago A, Ferrari E, Witkowski A, Wendler O, Kornowski R, Martinez- Clark P, Ciaburri D, Shemin R, Alnasser S, McAllister D, Bena M, Kerendi F, Pavlides G, Sobrinho JJ, Attizzani GF, George I, Nickenig G, Fassa AA, Cribier A, Bapat V, Feldman T, Rihal C, Vahanian A, Webb J, O’Neill W. Transcatheter mitral valve replacement in native mitral valve disease with severe mitral annular calcification: From the first multicenter global registry. JACC Cardiovasc Interv. 2016;9:1361–1371.11. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
