

Angiosarcoma: clinical and imaging features from head to toe
- PMID: 28471264
- PMCID: PMC5594986
- DOI: 10.1259/bjr.20170039
Angiosarcoma: clinical and imaging features from head to toe
Abstract
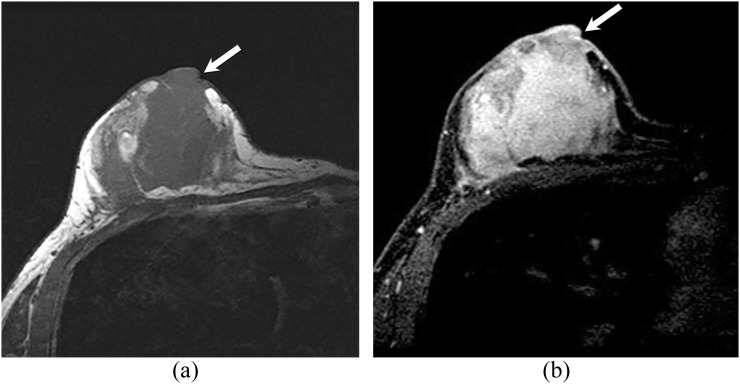
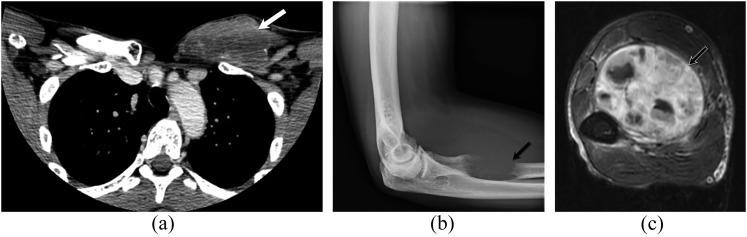
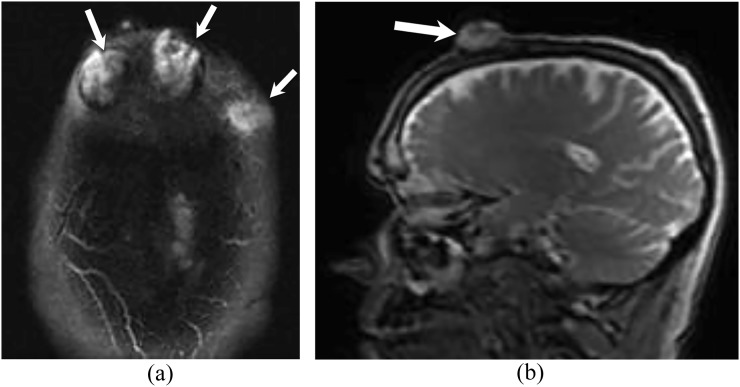
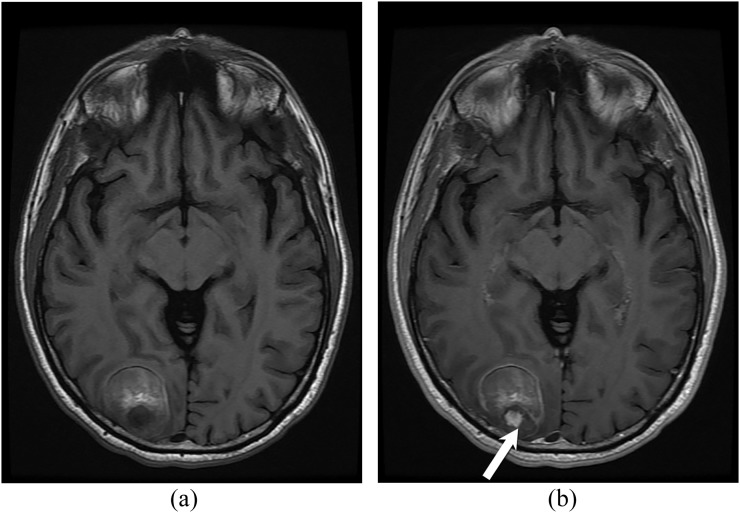
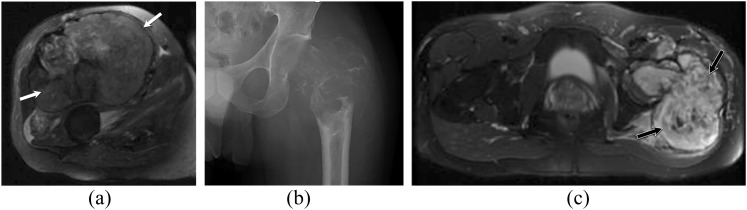
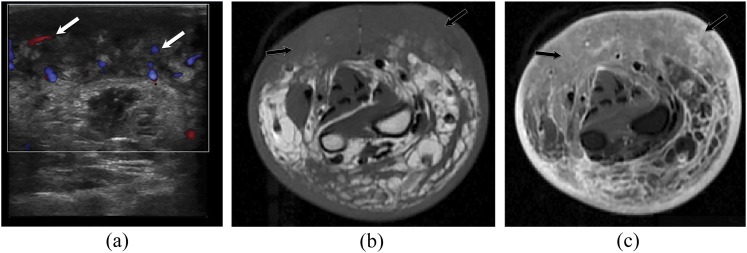
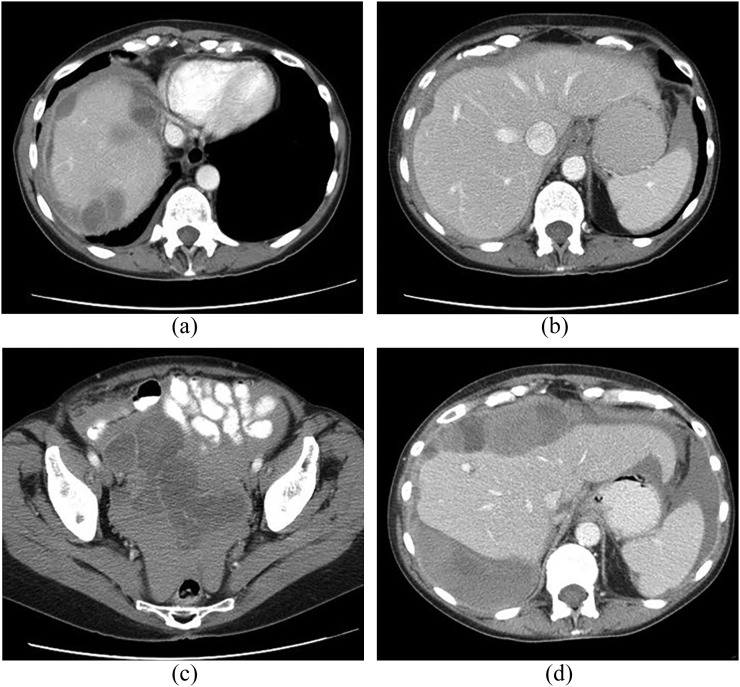
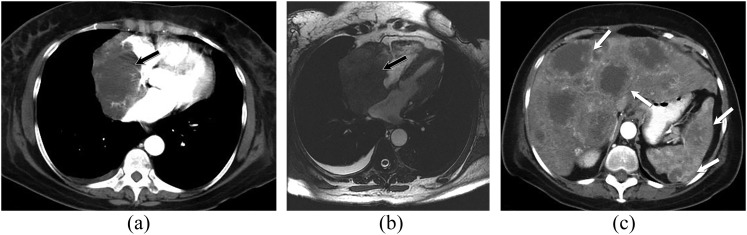
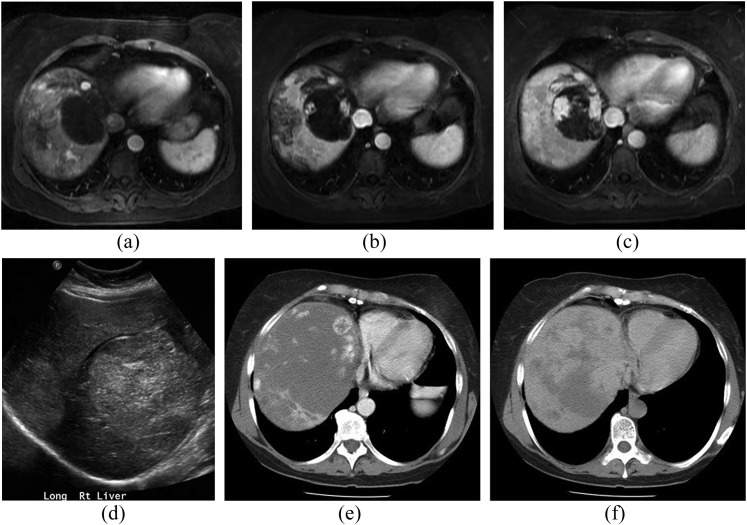
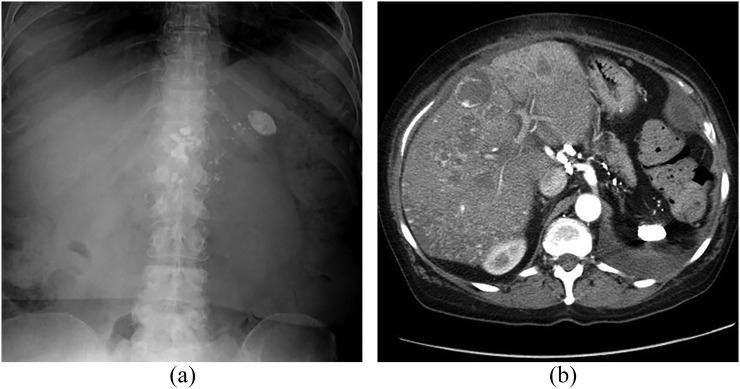
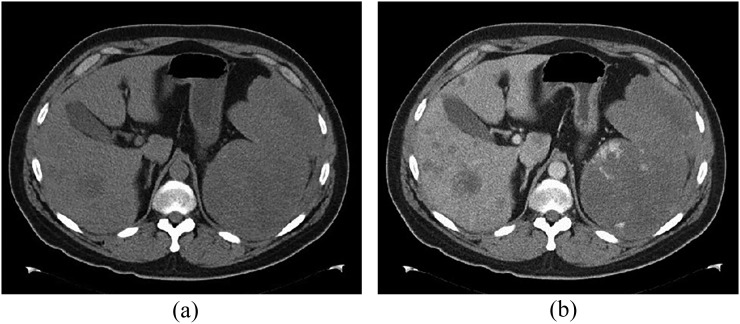
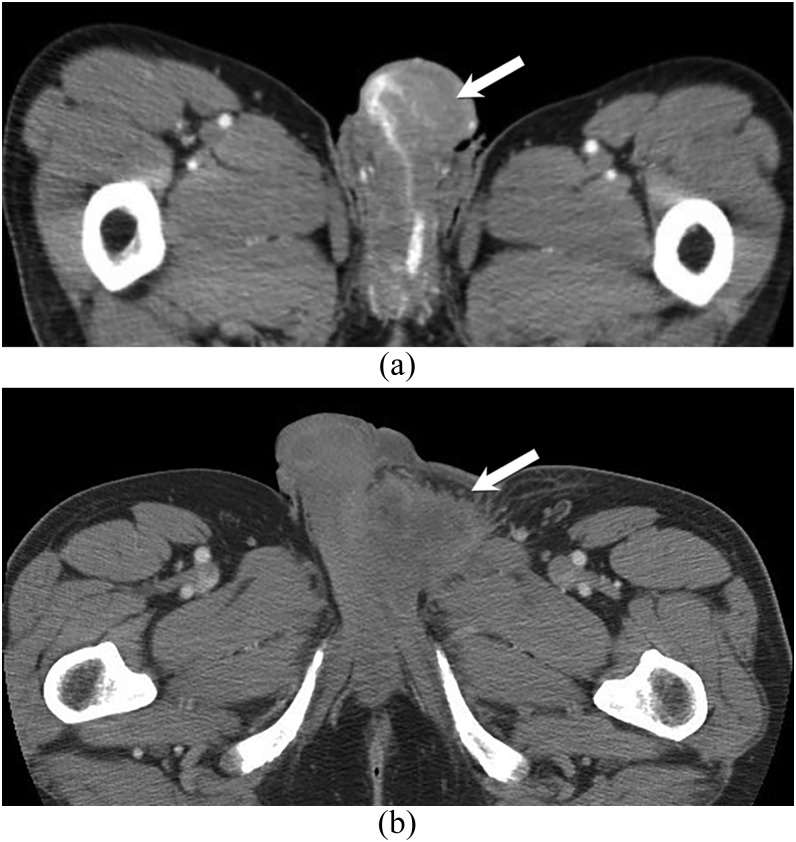
Angiosarcoma is a rare, aggressive subtype of soft-tissue sarcoma with a propensity for local recurrence and metastasis associated with a generally poor prognosis, unless diagnosed early. Given the vascular endothelial cell origin of angiosarcoma, tumours may develop in essentially any organ; however, there is a predilection for the skin where half of all tumours arise, increasing in prevalence with age. The most common risk factors are chronic lymphoedema and history of radiation. We review the most important radiological findings along the spectrum of angiosarcoma from head to toe throughout the body, including uncommon and rare locations. Key imaging features of angiosarcoma across multiple organ systems will be described, as well as the impact on management and prognosis.
Figures

References
-
- Peterson MS, Baron RL, Rankin SC. Hepatic angiosarcoma: findings on multiphasic contrast-enhanced helical CT do not mimic hepatic hemangioma. AJR Am J Roentgenol 2000; 175: 165–70. doi: https://doi.org/10.2214/ajr.175.1.1750165 - DOI - PubMed
-
- Walker EA, Song AJ, Murphey MD. Magnetic resonance imaging of soft-tissue masses. Semin Roentgenol 2010; 45: 277–97. doi: https://doi.org/10.1053/j.ro.2009.12.004 - DOI - PubMed
-
- Young RJ, Brown NJ, Reed MW, Hughes D, Woll PJ. Angiosarcoma. Lancet Oncol 2010; 11: 983–91. doi: https://doi.org/10.1016/s1470-2045(10)70023-1 - DOI - PubMed
-
- Walker EA, Salesky JS, Fenton ME, Murphey MD. Magnetic resonance imaging of malignant soft tissue neoplasms in the adult. Radiol Clin North Am 2011; 49: 1219–34, vi. doi: https://doi.org/10.1016/j.rcl.2011.07.006 - DOI - PubMed
-
- Murinello A, Mendonca P, Abreu A, Santos AL, Roquete J, Pinto E, et al. . Cardiac angiosarcoma—a review. Rev Port Cardiol 2007; 26: 577–84. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
