

Thromboembolic risk and effect of oral anticoagulation according to atrial fibrillation patterns: A systematic review and meta-analysis
- PMID: 28471498
- PMCID: PMC6490401
- DOI: 10.1002/clc.22701
Thromboembolic risk and effect of oral anticoagulation according to atrial fibrillation patterns: A systematic review and meta-analysis
Abstract
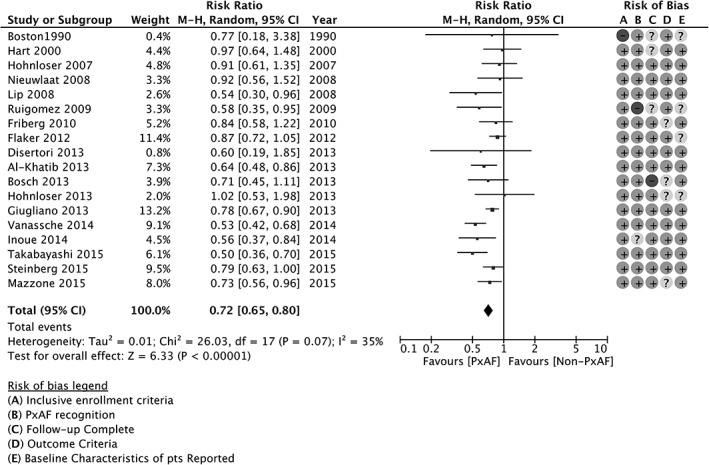
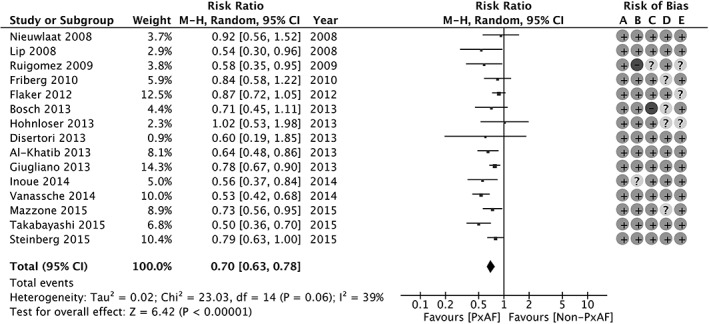
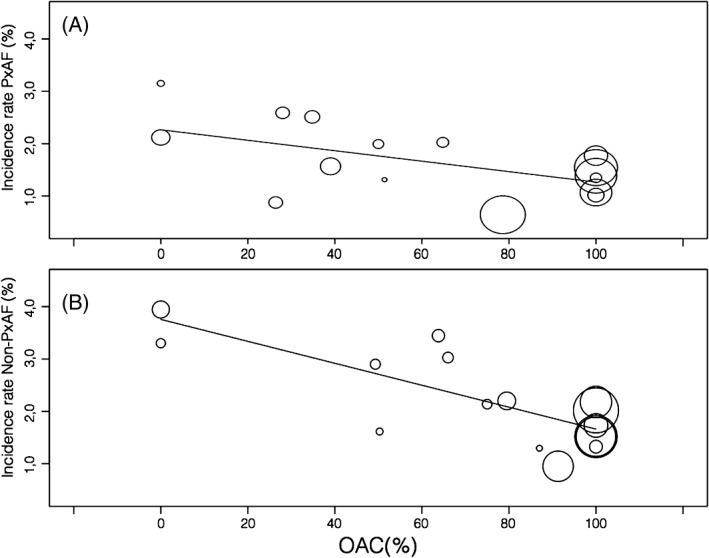
Oral anticoagulation (OAC) is recommended in both paroxysmal atrial fibrillation (pxAF) and nonparoxysmal AF (non-pxAF), but disagreement exists in classes of recommendation. Data on incidence/rate of stroke in pxAF are conflicting, and OAC is often underused in this population. The objectives of the meta-analysis were to investigate different impact on outcomes of pxAF and non-pxAF, with and without OAC. Two reviewers searched for prospective studies on risk of stroke and systemic embolism (SE) in pxAF and non-pxAF, with and without OAC. Quality of evidence was assessed according to GRADE approach. Stroke combined with SE was the main outcome. Meta-regression was performed to evaluate OAC effect on stroke and SE incidence rate. We identified 18 studies. For a total of 239 528 patient-years of follow-up. The incidence rate of stroke/SE was 1.6% (95% confidence interval [CI]: 1.3%-2.0%) in pxAF and 2.3% (95% CI: 2.0%-2.7%) in non-pxAF. Paroxysmal AF was associated with a lower risk of overall thromboembolic (TE) events (risk ratio: 0.72, 95% CI: 0.65-0.80, P < 0.00001) compared with non-pxAF. In both groups, the annual rate of TE events decreased as proportion of patients treated with OAC increased. Non-pxAF showed a reduction from 3.7% to 1.7% and pxAF from 2.5% to 1.2%. Major bleeding rates did not differ among groups. Stroke/SE risk is significantly lower, although clinically meaningful, in pxAF. OAC consistently reduces TE event rates across any AF pattern. As a whole, these data provide the evidence to warrant OAC irrespective of the AF pattern in most (virtually all) patients.
Keywords: Oral Anticoagulants; Paroxysmal Atrial Fibrillation; Stroke; Systemic Embolism.
© 2017 Wiley Periodicals, Inc.
Conflict of interest statement
The authors declare no potential conflicts of interest.
Figures
References
-
- Camm AJ, Kirchhof P, Lip GY, et al. Guidelines for the management of atrial fibrillation: the Task Force for the Management of Atrial Fibrillation of the European Society of Cardiology (ESC) [published correction appears in Eur Heart J. 2011;32:1172]. Eur Heart J . 2010;31:2369–2429. - PubMed
-
- January CT, Wann LS, Alpert JS, et al; ACC/AHA Task Force Members . 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines and the Heart Rhythm Society [published correction appears in Circulation. 2014;130:e272–e274]. Circulation. 2014;130:e199–e267. - PMC - PubMed
-
- Hylek EM, Go AS, Chang Y, et al. Effect of intensity of oral anticoagulation on stroke severity and mortality in atrial fibrillation. N Engl J Med. 2003;349:1019–1026. - PubMed
-
- Hart RG, Pearce LA, Aguilar MI. Meta‐analysis: antithrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146:857–867. - PubMed
-
- Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta‐analysis of randomized trials. Lancet. 2014;383:955–962. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
